Course
Georgia Renewal Bundle
Course Highlights
- In this course we will learn about the various communication types, threads, and barriers you will encounter during daily practice.
- You’ll also learn the basics of critical thinking education, followed by common exercises
- You’ll leave this course with a broader understanding of how to better apply nursing ethics into your daily practice.
About
Contact Hours Awarded: 30
Course By:
Multiple Authors
Begin Now
Read Course | Complete Survey | Claim Credit
➀ Read and Learn
The following course content
In this course, we will cover a variety of nursing topics which are listed in the course outline below. This course fulfills the Georgia Board of Nursing’s requirements needed for license renewal. Upon completion of this single module, you will receive a certificate for 30 contact hours.
Course Outline
- Key Concepts of Critical Thinking in Nursing
- Effective Communication in Nursing
- Ensuring Patient Confidentiality in Nursing
- Nursing Documentation 101
- Nursing Ethics
- Infection Control and Barrier Precautions
- PTSD in Nurses
- End of Life Process
- Sexual Harassment Prevention
- Following a DNR: An Ethical Dilemma in Nursing
- Screening for Suicide Risk Factors in Pediatrics
- Human Trafficking
- Pain Management in Nursing
- Drains: Everything you need to know
- Administration of Blood Products
- A Nurse’s Guide: How to Deal with Difficult Patients
Key Concepts of Critical Thinking in Nursing
How many times did you hear the phrase “critical thinking” in your training to become a nurse? I must have heard it a thousand times, and I still don’t think I ever had a clear definition of it in my mind. What exactly is critical thinking? In this course, we will answer those questions and provide insight into how you can teach critical thinking in nursing. Also included are some self-guided exercises to practice critical thinking skills. After all this, you will be ranting about the vital importance of critical thinking too.

Self Quiz
Ask yourself...
- How would you define critical thinking in your mind?
- Do you think of yourself as a critical thinker?
What is Critical Thinking?
Critical thinking is a term that is difficult to define because it is, by nature, somewhat subjective. The National Council for Excellence in Critical Thinking defines it as “the intellectually disciplined process of actively and skillfully conceptualizing, applying, analyzing, synthesizing, and/or evaluating information gathered from, or generated by, observation, experience, reflection, reasoning, or communication, as a guide to belief and action” (4). That’s a long definition. Essentially, critical thinking is a way of thinking that allows a person to recognize important information and process it to solve problems. Let us break this down further into the key characteristics of critical thinkers.
How are “text-book smart” and “street smart” different from each other?
Information Gathering
There are some key characteristics of critical thinkers that appear consistently throughout the literature. The first of these attributes is information gathering (1). Critical thinkers are adept at gathering information from situations. They pay attention to details and pick up on the information that others may miss. Critical thinkers try to uncover the particulars to ensure they are well informed in their thinking and decision-making. Critical thinking is not a passive acceptance of information but rather an active collection of data. In terms of nursing, the critical thinker will place a lot of importance on their assessment. Rather than focusing simply on the tasks that need to be completed, critical thinking in nursing means staying in tune with assessment findings and changes. For example, if a patient has labs drawn, the critically thinking nurse will watch for the results of these labs to have the most up-to-date information and be alert to any changes.
How do you incorporate “information gathering” into your routine?
Investigating
Another important attribute of critical thinkers is their habit of investigating (1). They do not accept information at face value. They have a tendency to question information, especially that which contradicts other data. When critical thinkers see the information that doesn’t seem right or raises questions, they investigate it. This way of thinking goes together with seeking out information.
With critical thinking in nursing, a nurse may ask themselves, “What else do I need to know? What comes next?” Rather than simply reporting one change to the physician, they think “what could this change represent? What other information would support this idea?” Continuing our example of following labs, if the nurse notices that the white blood cell count has increased, they will investigate to see why that might be. They would likely assess the patient for signs of infection, such as fever or chills.
If you get the feeling that “something isn’t right,” what do you do next?
Evaluation
Critical thinkers also can evaluate the information they have gathered to create new ideas or hypotheses (1). This is the cognitive “connecting the dots” that allows critical thinkers to synthesize pieces of data into a complete picture of what is happening.
Critical thinking in nursing doesn’t mean just collecting and reporting information; they process it and form ideas of their own. They ask questions like “how do these pieces of information fit together? Does this fit with any knowledge I already have?” Going back to our example, let’s say after the nurse notices the white blood cell count and assesses the patient, they find the patient has a fever and cloudy urine. Evaluation of this information would lead the nurse to think the patient has a urinary tract infection (UTI).
Think of a time you diagnosed a patient’s problem. How did you come to this conclusion?
Problem Solving
An important aspect of critical thinking is problem solving. After gathering and evaluating information, the critical thinker tries to solve any problems that surface (1). This is a key point that separates critical thinking from merely being perceptive. Recognizing important information and problems is vital but being able to then think through and solve the problem is what makes critical thinking stand out. Looking at our example again, once the nurse has recognized symptoms consistent with a UTI they will begin formulating ideas on how to treat the problem. The first action would likely be notifying the provider of all the information gathered, the nurse’s hypothesis and a recommendation to solve the problem. You may recognize this format as being similar to Situation-Background-Assessment-Recommendation (SBAR). SBAR is a tool that is used to help guide critical thinking in nursing (1).
Self Quiz
Ask yourself...
- What information/assessments do you focus on for the patients you care for?
- What characteristics do you think a critical thinker should have?
- Have you recognized patterns in how your providers/institution solve common problems?
- Have you ever had a provider recommend a treatment you disagree with? Why did you disagree?
- What information/assessments do you focus on for the patients you care for?
- What characteristics do you think a critical thinker should have?
- Have you recognized patterns in how your providers/institution solve common problems?
- Have you ever had a provider recommend a treatment you disagree with? Why did you disagree?
Why is Critical Thinking Important?
Now that we understand what exactly critical thinking means, let’s ask: why is it so important? You may have already formulated some ideas about how critical thinking in nursing can be helpful in practice. Critical thinking is a pattern of recognizing and reacting to the most important pieces of information. This is crucial in nursing, where we are presented with a plethora of information and expected to use the most important pieces to save lives and make people healthy. Now, let us get more specific on what areas would benefit from critical thinking in nursing.
Patient Outcomes
First, and maybe most important, is that critical thinking improves patient outcomes (3).
Studies have shown that critical thinking skills in nurses are linked to lower hospital costs to patients, as well as to the facility thanks to lower in-hospital complications (3). Critical thinking by nurses also decreases the length of hospital stay (4). It has also been shown to improve outcomes and lower complications in surgical patients when the operating room nurses had a higher level of critical thinking (3). Despite these positive results and every nursing instructor ranting on the importance of critical thinking, there is a lack of research into the connection between critical thinking in nursing and patient outcomes. This is primarily because of the difficulty of assessing critical thinking skills specific to nurses and linking these skills to a measurable outcome without confounding factors (3).
Staff Satisfaction
You will be pleasantly surprised to learn that critical thinking in nursing leads to higher staff satisfaction! Research has found a strong correlation between critical thinking ability and perceived autonomy and job satisfaction in nurses (5). It is believed that critical thinking fosters autonomy or at least increases the sense of autonomy, which generally leads to higher job satisfaction. Critical thinking has been shown to improve confidence as well, and feeling confident in your work generally improves satisfaction as well (5). Interestingly, there has also been research that shows that critical thinking is linked to higher satisfaction with life decisions and less adverse life events (6). The idea here is that critically thinking through a decision before making it leads to less regret. So, this course will make you happier with work and help you make better life choices – you’re welcome.
Efficiency
Another important benefit of critical thinking is that it improves efficiency. Studies found that nurses with higher critical thinking skills work more efficiently (1). If you are thinking critically you are better able to prioritize and plan to avoid wasting time and energy. As we all know, nursing can be very demanding, and efficiency is important for tending to all our patients’ needs. Also, if the nurse manager of a unit has higher critical thinking skills, they implement changes that improve overall efficiency and morale (7). This highlights that critical thinking is important to all nursing forms and how one person practicing critical thinking can impact others.
Healthcare Complexity
A large reason why critical thinking has become so important is the ever-increasing complexity of healthcare. As we develop new treatments, we are always being asked to learn new processes and how to monitor patients receiving these treatments. Also, as the healthcare system improves treatments, the average patient is becoming older and has more co-morbidities (4). This adds to the complexity of each patient. Critical thinking is a great skill that aids in learning new tasks and comprehending more complicated patients. Nurses arguably have the most complex set of tasks, as we are often asked to perform some of the duties of other healthcare professions. Being adaptable to whatever changes come and taking on new responsibilities is a great benefit of critical thinking.

Self Quiz
Ask yourself...
- Have you ever seen a colleague miss something that may have harmed the patient?
- Have you or a colleague ever had a “good catch” that you feel benefited the patient?
- How do you think critical thinking increases autonomy?
-
When have you been asked to make a change to your practice? How did you adapt to this change?
- How could you make your work routine more efficient?
Critical Thinking Education
Now that we understand what critical thinking is and why it’s important let us discuss how critical thinking is taught. Critical thinking in nursing has become an integral part of many programs. Many healthcare institutions are looking for ways to incorporate critical thinking into their training process as well (1). Critical thinking is, however, an abstract concept and truly is a whole new way of thinking. So, how do we teach someone how to think? There are several factors that should be considered when trying to teach or learn critical thinking.
Educator Influence
First, educators have an important influence on the instruction of critical thinking skills. Educators that are effective at teaching critical thinking skills are open-minded, flexible, and supportive of their students (1). Showing flexibility and not firmly holding to one set way of doing things allows the students to adopt their own version of critical thinking. Role-modeling, guiding, and being knowledgeable about critical thinking also leads to a more effective educator (1). The educator should guide learners through their understanding of critical thinking while role-modeling critical thinking behaviors.
Environment
The learning environment also plays an important role in a nurse’s ability to learn critical thinking skills. The environment should be inclusive, non-judgmental, and allow for open discussion (1). This applies to both nursing schools and nurses being trained into a new unit. Feeling accepted on a unit allows for better learning and has a positive impact on critical thinking skills (1). It is important for nurses looking for a new work unit to find one with a welcoming, safe environment to aid in learning. On the other side, we should always strive as nurses to be inclusive and facilitate this type of environment as it benefits everyone. I was always told that “nurses eat their young,” and this attitude does not foster learning or growth.
Education System
The education system also impacts the teaching of critical thinking. Education systems, for one, largely shape the learning environment and educators. The education system should strive to create the type of learning environment where critical thinking skills can grow. Too much emphasis on classroom lectures and power dynamics between teachers and students hinders the development of critical thinking skills (1). Teaching critical thinking as its own subject also helps students learn the skill (1).
Individual Factors
Lastly, there are some individual factors that affect a person’s ability to cultivate critical thinking skills. Chief among these are a lack of confidence and fear of questioning an instructor (1). You can see how all these concepts seem to be centered on the fact that learners perform best when they are comfortable and have the freedom to discuss ideas. This is the central concept that should be understood and practiced by both mentor and mentee, as well as the education system as a whole. So, as we move into the next section teaching critical thinking skills, put yourself in a comfortable place – physically and mentally. Be sure to keep thinking of questions and follow your own ideas.

Self Quiz
Ask yourself...
- What training or education did you receive on critical thinking?
- Who was your favorite instructor/mentor? What did they do to stand apart from others?
- What factors make you more comfortable and likely to learn?
- What were the dynamics like at your nursing school?
- Have you ever felt afraid of asking a 'stupid' question?
Strategies to Promote Critical Thinking
Now that we have an understanding of the right mindset to have when learning critical thinking, let us actually discover how to teach and learn it. Some common strategies that appear to be effective are targeted questioning, case studies and simulation (1). These are all approaches that require more than one person, so they are best practiced as part of training. If you have a colleague or mentor, you may try some of these strategies with them as well.
Targeted Questioning
First, we have targeted questioning, which is a tactic of asking questions in order to promote further thinking (8). This often involves asking questions of increasing difficulty to encourage the learner to think deeper about what the facts represent. It is the educator’s equivalent of a toddler asking “why?” over and over. The purpose is not to be annoying but to discover how deep down the rabbit hole the learner will go. Socratic questioning is another common type of targeted questioning designed to encourage learners to think further on the subject matter. This is commonly used in continuing education (check the italicized text), and helps to promote further thinking on facts rather than just accepting them at face value.
Case Studies
The next exercise that helps teach critical thinking is case studies. Case studies help promote critical thinking by allowing learners to think through a real-life scenario without the stressors of experiencing the scenario (1).
It is important for learners to acknowledge how they might feel in that scenario so that they can be better prepared for the pragmatic aspects and the personal aspects of dealing with the presented problem (4). Case studies typically move chronologically through a scenario and often guide learners through the critical thinking behaviors of information gathering, investigating, evaluating and problem-solving. This helps build the mental framework of moving step-wise through a problem in order to find the best solution.
Simulation
Finally, simulation has proven to be useful in fostering critical thinking. Simulation, similar to case studies, promotes thinking through a scenario in a low-risk, low-stress environment with the added benefit of going through the physical motions involved (8). This allows the learner to physically experience the situation as well as think through the problems. This can help familiarize someone with the actual physical interventions involved so they are more comfortable when practiced in real scenarios. This is often used in life support training so that learners understand how to actually connect the defibrillator and which button to press, so there is less fumbling in the high-stress scenario where these motions are used (8).
Self Quiz
Ask yourself...
- Did you ever have an instructor “grill” you on facts? What did this do for your learning?
- Have you ever found yourself comparing a problem to a similar previous problem?
- What is your experience with simulation?
- Think of a stressful situation you were confronted with at work. Could that situation be captured in a simulation?
Critical Thinking Exercises
We have examined ways to teach critical thinking skills to others, but what about developing critical thinking within ourselves? Luckily, there are a couple of exercises that can be practiced individually to foster critical thinking skills. This is helpful to those of us who are finished with our training and looking to better ourselves. Start with a desire to improve, as none of us are perfect. These exercises are best practiced by focusing on a specific scenario, particularly if there is a scenario that you didn’t fully grasp or that felt overwhelming.
Concept Mapping
The first exercise is concept mapping. Concept mapping is the practice of visually representing ideas on paper and showing connections between these ideas (2). They are often presented in either a hierarchical or web pattern with the key ideas at the top or center of the diagram, respectively.
This helps a learner visualize their thinking process and further think about what connected and how. For example, let's think of our scenario earlier with the suspected UTI. We might see a change in vital signs as a central idea which connects us to signs of infection and then to interventions. This can help us see the progression of ideas, how they are connected, and possible other explanations.
Reflective Writing
Our final means of learning critical thinking in nursing is reflective writing. Reflective writing or journaling helps to identify thought patterns and promote critical thinking skills (1). Again, this is most useful for examining a specific situation. Breaking down a complex situation when you have more time to analyze it will help you learn more from that challenge.
It may seem silly to write a journal but reflecting and processing your ideas is an important practice for growth. The act of formulating your thoughts into written words helps to make more sense of the ideas and feelings you have. You don’t have to keep a daily journal, but if you have a challenging shift it may help to reflect on it and write down your ideas. It is important to treat this exercise as a learning opportunity, and to not ruminate on failures or beat yourself up for not being perfect.

Self Quiz
Ask yourself...
- Practice drawing a concept map of the key concepts of critical thinking from this course.
- Write down a tough scenario you have dealt with at work. What made this experience hard?
- How have you or will you change your practice based on this scenario?
Conclusion
In summary, critical thinking in nursing is essential. It impacts our efficiency, the well-being of our patients, and our own happiness. Critical thinking is a broad way of thinking that involves gathering information, investigating, and evaluating the information in order to solve a problem. Critical thinking is best learned and practiced with an open mind. We can foster critical thinking in each other through case studies, simulations and targeted questioning. We can improve our critical thinking in nursing skills ourselves by practicing reflective writing and concept mapping. If you are a nurse educator or preceptor, I hope you have found something you can use to shape future nurses. If you are a nurse looking to better understand critical thinking, I hope you have learned something you can take to your nursing practice.
Effective Communication in Nursing
Introduction
Communication in nursing is key, and the ability to communicate effectively can be our lifeline. We depend on ourself and others to be fluent and effective in the art of communication in order to perform our role as nurses successfully. When any link in our communication chain fails, we immediately see poor outcomes, wastage of resources, reductions in patient and staff satisfaction as well as a decline in the quality of patient care (1).
Types of Communication
In order to master effective communication in nursing, it is important to understand the various types of communication, their definitions and the impact they can make.
Non-Verbal
This form of communication relies solely on body language, including body and facial mannerisms, and lacks spoken words or sounds (2, 3). We perform and identify non-verbal communication in nursing daily without giving it a second thought. We may see a newborn sucking on their hands, providing us a non-verbal cue that they are hungry. When assessing a patient holding their abdomen, we would initially target that area because they have communicated (non-verbally) that this is where they are experiencing discomfort. Smiling when the next shift nurse walks in the door communicates to them that you are happy to see them and that it's about time to go home!
Since we perform non-verbal communication so often, it can become a potent or extremely damaging tool. This form of communication in nursing can be used positively to show our patients and co-workers that we have compassion and are engaged. Negative forms can make patients uncomfortable with sharing their medical history and result in a lower quality of patient care. Additionally, it can lead to dysfunctional teamwork among staff (2).
Verbal
Verbal communication occurs when we use words or sounds to discuss concepts with others (2). This form of communication in nursing has the conception to be a very easy notion, but it can create unfavorable consequences when used ineffectively. In order to produce clear verbal messages, we should always speak concisely and confidently. As healthcare professionals, we have our language and understanding of when to incorporate medical jargon into conversations versus when not, which is crucial in providing care (4). When communicating among co-workers, our medical knowledge can display professionalism, and they can follow along. However, when speaking with patients and their families, this may only sometimes be the case, and we must be able to effectively gauge our audience and ensure that they clearly understand what we are teaching or explaining; this is a precious tool.
Written
This form of communication can be either a formal or informal transcription of words intended to serve as a direct communication form (2). Written communication in nursing is used daily and incorporates one of our most essential duties: documentation. Throughout our nursing practice, we have learned the importance and necessity of our documentation; it can be helpful for legal protection or provide critical data to other healthcare professionals. Written communication can also be accessed through our policies and procedures to perform various tasks. Having sound, written communication and interpretation skills is vital to the overall success of our nursing career.
Self Quiz
Ask yourself...
-
What type of communication is being interpreted while watching a patient walk to the bathroom?
-
Upon admission of a female patient for a fall, you are performing normal intake questions and a physical assessment. The patient is quiet and uses minimal verbal communication and looks down at the floor while you are in the room. What communication types are you interpreting?
Receiving Communication
The most common communication perception is usually directed at producing communication through non-verbal, verbal, or written forms. While the production of communication is essential, the reception of it holds even greater value. In nursing, ensuring our communication is received correctly affects every clinical, orientation, or job experience we have encountered thus far. Think about it...
- I was taking notes in class or during a shift.
- When a preceptor or instructor educates you on a new skill or equipment.
- You teach your patient, family, or student about a new diagnosis.
- You are watching your patient breathe for rate, depth, and effort.
We must successfully provide and receive communication in nursing through verbal, non-verbal, or written forms. If communication fails, we will experience highly adverse effects throughout our nursing system (2).
Hearing & Listening
Hearing describes the process or act of perceiving sounds or spoken words (2). We hear sounds upon auscultation, varying frequencies of alarms, and patient concerns when voiced. Hearing all these sounds is heavily dependent on how they are used. We must also listen to these sounds and words to successfully implement these sounds. To listen, we must hear and then interpret these sounds carefully (2). We interpret these sounds and words by asking additional questions, performing additional assessments, or paraphrasing the information presented.
Active listening is when the listener understands the information discussed and provides feedback (5). Ways to ensure active listening are having the patient repeat the information in their own words and paraphrasing it. Active listening patients may also ask questions relevant to the topic discussed. Some additional tips to ensure active listening and participation are providing the environment is free from distractions or biases, making eye contact, and allowing the speaker to fully respond before interrupting (5).
Self Quiz
Ask yourself...
- What is the best way to ensure a patient was actively listening while performing patient education?
- Which type of scenario requires active listening skills?
a. Putting blood tubing into a pump.
b. Watching a EKG monitor.
c. Performing a pain assessment. - What techniques show others you are actively listening?
a. Reading a document while being talked to.
b. Making eye contact.
c. Making noises while someone is talking.
Communication Transmission Threads
Communication in nursing occurs multiple times a day between a wide range of communication threads. The type of communication through non-verbal, verbal, and written communication produced and received must be effectively performed (4). Success and implementation depend heavily on the communication between the nurse and the communication thread.
Nurse - Nurse
Communication among nurses is continuous throughout a shift while working within a team environment. Whether we pass our documentation on to another nurse for review or vice versa, there is a consistent, communicative flow of all variants (non-verbal, verbal, and written) between the team to provide patient care. Another way to effectively communicate patient information is to use a structured communication framework, such as the situation, background, assessment, and recommendation (SBAR) format.
Nurse - Ancillary Staff
Your team members will vary depending on your nursing career setting, but some items will remain consistently critical wherever you are. We must communicate clearly when delegating or reporting essential information from the nurse to ancillary staff participating in patient, client, or resident care.
Charge Nurse - Team
There will always be unexpected tasks, staff conflicts, or emergent situations when stepping into a charge nurse role. In this position, you will be putting all the communication skills you have acquired into practice at an all-time high. As the charge nurse, you will be viewed as a leader, meaning you are a role model for your team members. Now, in addition to effectively producing and receiving communication, you will identify poor communication and assist with its correction.
Nurse - Patient
The nurse-to-patient communication thread is one of the ultimate and most essential exchanges in the nursing profession (4). Patients need us, so we must maintain consistent and effective communication with them because any assessment, report, or medication administration is contingent upon it. Additionally, bedside patient reports during shift change are valuable to ensure effective nurse-patient communication.
Nurse - Family
The thread between the nurse and the patient’s family can be the foundation for your nurse-to-patient communication and its effectiveness. The family could be the responsible party or guardian for your patient. It could serve as your sole historian for patient information if the patient cannot communicate at the time of data collection. Ensuring that the family is aware of and understands discharge instructions can help them recognize any potential signs or symptoms that could result in calling a physician or visiting the emergency room.
Self Quiz
Ask yourself...
- Which of the following is a beneficial way to ensure effective communication throughout multiple threads?
a. One to one conversations.
b. Reviewing a policy.
c. Bedside report.
Barriers & Improvements to Communication in Nursing
Barriers to communication in nursing happen frequently and are sometimes out of our control. These barriers include:
Environmental-related barriers
When providing patient education, the surrounding environment can negatively impact effective communication. Alarms, noisy surroundings, lack of privacy, and lighting can all be distractions when fostering a positive learning environment (6). As nurses, we must try to teach patients in an optimal environment conducive to listening and learning as much as possible.
Cultural differences
Identifying cultural differences during admission and cultural awareness will allow effective communication management throughout each culture you are presented with (6). Nurses must acknowledge their personal and cultural beliefs and differences. Additionally, they should respect patients’ cultural differences and refrain from judgment.
Healthcare Institutional BarriersPatient acuity, low staffing levels, and time constraints can contribute to communication barriers (6). Nurses can improve these barriers by utilizing staff huddles and working with the administration to overcome high-acuity patient assignments and some time constraints. Nurses may utilize a patient-centered approach and prioritize patient communication over routine tasks to improve communication.
Emergent situations
Emergent situations during your shift can be relieved through adequate knowledge of the policies and procedures and by performing debriefs after the problem is resolved. Debriefings hold valuable insight into reflections on the emergent situations we face as nurses, especially on communication performance.
In each thread and form of communication in nursing, we must remember the following items to receive information. While producing communication, we must always be clear, concise, and accurate with the correct corresponding tone when expressed to others. When we receive information, we must ensure we understand, investigate, and act according to the communication presented. Utilizing various communication platforms, including emails, boards, and group messaging apps, can help to ensure education is received.
Benefits of Effective Communication in Nursing
When we achieve effective and therapeutic communication between both our team and patients, it will create opportunities for enhancements throughout our practice. Fostering a unity of teamwork with co-workers will increase satisfaction and reduce burnout rates. Reduced health care costs through reduced readmissions or emergency room visits will be established by successful patient education and understanding. Our quality of patient care will be heavily influenced by the nursing communication threads created through their care.
Ensuring Patient Confidentiality in Nursing
Introduction
In order to provide the best care possible to patients, there must be a foundation of trust that the patient-provider relationship is built on. If the foundation is not stable, the rest of the relationship is at risk of crumbling. One way that trust is built is by maintaining patient confidentiality or privacy.
When it comes to the medical field, the wrong medicines or treatments may be administered or performed. This could result in further complications. Medical conditions, treatments, and results can often be sensitive topics patients do not necessarily want shared with society for a variety of reasons. Patients rely on their providers to keep the information they communicate in confidence, only sharing under certain circumstances.
With the ever-growing platform of social media and advancements in technology, there is a gray area that exists when it comes to patient confidentiality and what can and cannot be shared. The purpose of this course is to educate learners on aspects of patient confidentiality and its importance.
Self Quiz
Ask yourself...
- What do you already know about patient confidentiality?
The Privacy Rule
The Health Information Portability and Accountability Act of 1996 (HIPAA) became the groundwork for the Standards for Privacy of Individually Identifiable Health Information (Privacy Rule) issued by the U.S. Department of Health and Human Services (HHS). It was designed to meet the requirements set by HIPAA regarding how healthcare providers used and disclosed a patient's private health information. It also addressed patients having the right to know and dictate how their health information is utilized. Overall, the Privacy Rule's goal was to set clear boundaries when it came to properly protecting health care information while allowing the exchange of pertinent information to protect the health and well-being of the public (2).
Many groups are included under HIPAA's term of "covered entities.” These entities have connections to personal health care information on a variety of levels. Groups such as healthcare providers, health plans, healthcare clearinghouses, and business associates are all covered entities. The protected information they encounter is anything that can or is believed to identify an individual: name, date of birth, address, and Social Security number. Any past, present, or future mental or physical health, condition, or payment and health care provisions for an individual are also classified as protected information (4).
Self Quiz
Ask yourself...
Think of where you work.
- What type of facility do you work in?
- What does your work consider patient identifiers?
- Is there anything you think should be added to that list when it comes to what can identify a patient?
De-Identifying Patients to Ensure Patient Confidentiality
There are many steps involved in de-identifying a patient for those who use or share patient information, as it applies to HIPAA. De-identifying a patient is the act of removing as many identifiers as one can in order to eliminate the chances of an individual being recognized through the scenario or situation (3). The following are two methods of de-identification.
Formal Evaluation by a Qualified Expert
A qualified expert must be a person with significant knowledge and experience in scientific and statistical standards or methods to ensure patient information is not identifiable. They do this by determining if the risk of using the information is very small. They often document what methods they use to make the determination (3).
Removing Individual Identifiers
Many identifiers are things one would expect to be removed when identifying a patient, such as a name, age, date of birth, home address, Social Security number, full-face photos, and phone numbers. However, some include any form of vehicle identifier (serial or license plate number), internet protocol (IP) addresses, biometric identifiers like finger or voiceprints, serial numbers or device identifiers, and web universal resource locators (URLs). An entire list of the 18 identifiers is located on the Department of Health and Human Services website (3).
Neither of these methods are 100% perfect in their goal, but they decrease a patient's chance of being identified significantly. Once the patient has been de-identified, the information is no longer restricted by the Privacy Rule since all patient identifiers have been removed. This means that the information can be used without worry of violation (3).

Self Quiz
Ask yourself...
- Which version of de-identifying a patient do you think is better?
- Have you ever had to de-identify a patient or patients?
- What was it for?
- Did you expect some of the listed identifiers to be on the list?
Professional Statements
Over the years, professional medical organizations have released statements regarding patient confidentiality and how it pertains to their target audience. Many medical organizations such as the American Nurses Association (ANA) and the American Medical Associations (AMA) often create position statements to reflect the organization's overall stance and thoughts on a specific topic. These positions may be used to guide education, policies, or individual opinions on the topic.
The ANA released a statement regarding patient privacy and confidentiality. As mentioned before, the ANA believes that the patient-provider relationship is important, and confidentiality is essential in that relationship. The organization supports legislation, standards, and policies that protect patient information. In the professional statement document, the ANA goes on to give the following recommendations regarding the protection of patient information (1, para 3).
- “Nurses should advocate for policies that ensure individuals’ right to privacy and protect against unwanted, unnecessary, or unwarranted intrusion into a person’s life.”
- “In the course of advocating for patients, nurses act to ensure privacy in the care environment as fully as possible so that patient privacy and confidentiality can be maintained.”
- “The patient’s right to confidentiality of individually identifiable health information is established statutorily with specific exceptions. Nurses should follow organizational policies that safeguard an individual’s right to decide to whom, the extent, and under what circumstances their individually identifiable health information will be disclosed.”
- “Violations of privacy and breaches of confidentiality threaten patient welfare. Nurses act to address practices and behaviors that risk patients’ privacy and confidentiality, escalating the concern as necessary per organizational policy.”
- “Confidentiality protections should extend not only to health records but also to other individually identifiable health information, including oral reporting, clinical research records, images, and mental health and substance use disorder therapy/treatment notes. This protection should be maintained in the treatment setting and in all other venues.”
- “Patients should receive accurate information regarding federal legislation (e.g., HIPAA, the Genetic Information Nondiscrimination Act [GINA], and the 21st Century Cures Act) that addresses individually identifiable health information and any limitations, exceptions, or implications associated with legislation affecting the right to privacy and confidentiality.”
- There is a heavy emphasis on not using patient information if consent has not been given unless there is an extenuating circumstance regarding legal requirements. This will be discussed in the next section.
Since patient confidentiality is extremely important, the ANA supports healthcare organizations in creating safeguards to protect patient confidentiality. They also support the organizations enforcing ways to alleviate violations by health care workers and protect them from retaliation (1).
Self Quiz
Ask yourself...
- Have you read the ANA's statement on patient confidentiality before?
- Are you in any professional organizations?
- Do these organizations have any statements about patient confidentiality?
- Are there any differences between them and the ANA's statement?
Disclosure
Overall, patient information is discouraged from being shared; however, there are several instances where the sharing of information is allowed. The patient may give the provider(s) or healthcare organization permission to share the information with whoever the patient decides (6). By providing consent, the patient is essentially waving the right to keep that information confidential but determines who can receive the information. This can be done through written or verbal consent, though most facilities require a written one. This written form is placed in the patient's medical records.
If another healthcare agency or provider is going to be involved with the patient's care, medical information can be exchanged on a "need to know" basis (6). For example, if a patient is being transferred to another facility, the accepting nurse and care team would need a thorough report to ensure that they knew the patient and what had already been done for them regarding medical care.
While protecting patient information is important, there are a few circumstances—called extenuating circumstances—that allow healthcare providers to share information regarding a patient without permission outside of the above reasons. Certain information is required to be reported to public health departments or authoritative organizations: communicable diseases, suspected child or elder abuse, gunshot wounds, release to insurance companies for payment, or worker's compensation boards after a claim has been submitted are allowed (8, 9).
In the case of protecting the public, healthcare providers can report patient information to a specific organization if it comes down to the health of the public. As mentioned above, testing positive for communicable diseases can be reported to public health departments.
It should be noted that one important exception applies to this rule. Making assumptions, especially about if a spouse has the right to know the medical history of a patient just because they are married, is not advised. Patients should be encouraged to inform their spouse about the information that may put the spouse at risk, such as sexually transmitted infections. If the individual's direct safety is threatened, then the provider can tell them (2).
In order to protect society, healthcare providers have the duty to warn if they have detailed and documented proof that the patient is targeting a select individual or group. Providers are encouraged to document instances of threats, whether it be against them, another provider, or another individual outside of the healthcare setting. Often this is a legal or ethical duty to report the threat to the authorities or possibly warn the potential victim (2).
If a provider is concerned about what can or cannot be disclosed at any time, it is encouraged that the provider consults hospital policies before releasing any information.
Self Quiz
Ask yourself...
- How do you obtain consent for sharing information?
- Have you ever shared information outside of the "need to know" basis with other providers when it comes to a patient?
- Have you ever had to report a patient to another organization such as Child Protective Services or the county Department of Health?
- What was it for?
Consequences of Disclosure Violations
Healthcare providers may be subjected to a variety of consequences when it comes to the violation of HIPAA or the Privacy Rule. The healthcare provider and the facility in which they work may be subjected to civil suits in a variety of ways (6). Disclosing sensitive information or photos about the patient is a breach of legal duty—intentional or unintentional. Nurses may face disciplinary action from their state's board of nursing. With the ever-growing form of social media, boards of nursing have been cracking down on improper use of social media and breaches in patient confidentiality. Job loss and fines are other consequences that may occur by themselves or in addition to any of the others listed above (6).

Self Quiz
Ask yourself...
Think back to your hospital policies.
- Do you recall any consequences listed in the policy?
- Are you required to complete education regarding patient confidentiality at work?
- What kinds of consequences do you think would be appropriate for violating patient confidentiality?
- What do you think of healthcare providers using social media at work?
Patient Confidentiality in the Technology Era
There are many forms of technology today and there are many ways patient confidentiality can be violated by using it. Cell phones have become a staple in nearly everyone's day-to-day life, so it would make sense that both healthcare providers and patients alike have them. While they are useful, cell phones can also cause problems. Unintentional or intentional filming or recording of patients or medical information can happen by staff, family members, or other patients. Family members or friends may call to ask about a patient, and it is important for the nurse to know hospital policy when it comes to verifying the identity of those calling and what information can be given over the phone. Verifying with the patient who can be told what information is important as well (6).
Since charting has become electronic, many nurses are using computers, laptops, or tablets to complete their charting. Healthcare providers need to ensure that privacy is always maintained when utilizing these devices.
Even though most things can be transferred via email, call, or secured text message, some information still needs to be transmitted via fax machine. Since there is room for human error, coversheets should be used along with a clear identifier that the information being sent is confidential (6). If a number is used often, it is encouraged that it is preprogrammed into the fax machine to help decrease the chance of the number being mistyped (7).
Self Quiz
Ask yourself...
Think of your work area.
- What types of devices does your facility to use to chart?
- What steps has the facility taken to protect patient information when it comes to these devices?
- What steps do you take to protect patient information?
- What things could be improved on when it comes to securing patient information?
Best Practices of Patient Confidentiality
Overall, healthcare providers must make decisions on how to protect private information. Despite recommendations from professional organizations and policies from facilities, it is the provider's responsibility and decision on how to go about it. Sometimes there are several ways to solve the same problem. Best practices, like the ones listed below, can be used with hospital and Board of Nursing policies and rules (6).
- Utilize coversheets for person notes regarding patient care or when faxing sensitive information.
- Be mindful of what is said in semi-private rooms or rooms that have visitors. Curtains and walls are not soundproof.
- Verify callers before providing any patient information as determined by hospital policy. Remember to also verify with the patient if able to do so. Some patients may not want family or friends to know about their condition.
- Do not leave patient information in a place where it can be easily seen by others. This includes personal notes, electronic or printed medical records, unlocked communication devices, etc.
- Ensure that all patient information is properly disposed of or destroyed prior to leaving work.
- Be mindful of what is posted on social media and be aware of possible unintentional disclosure.
- Provide education to staff regarding potential areas of misuse when it comes to patient information. Policies regarding improper use should be implemented. These policies should include email use, personal electronic data devices, and electronic transmission of data.
- Have staff and others who may need access to patient information such as students sign confidentiality agreements.
- Refrain from speaking about patients or their private information in areas where information can be overheard, such as cafeterias, hallways, elevators, waiting rooms.
- Ensure that policies are reviewed and updated periodically or as needed to reflect current healthcare laws and guidelines.
This is not a comprehensive list, and healthcare providers must use common sense and caution when sharing private patient information.
Self Quiz
Ask yourself...
- From the above list, what do you already do to protect patient information?
- From this list, what would you add to your own list?
- What would you add to this list regarding protection of sensitive information?
- In your workplace, where can you find information about privacy laws?
Conclusion
The topic of patient confidentiality is very important to the patient-provider relationship. Without it, the entire relationship can deteriorate, leading to significant emotional and possibly physical damage. This can be detrimental to the patient and provider. It is important to follow hospital policy and healthcare laws regarding sensitive information. All healthcare providers are strongly encouraged to stay up to date on new legislation that may affect patient confidentiality.
Nursing Documentation 101
Nursing documentation is at best a useful tool for communication and at worst a necessary evil. It is well-known that documenting is one of the most tedious aspects of bedside nursing. It takes time away from patient care and may be used for (or against) you in court. In this CE module we will learn how to document properly. Proper documentation is an essential for defense against claims and continuity/quality of care in nursing.
Introduction to Nursing Documentation
“I just love charting,” said no nurse, ever. If you ask most people why they want a career in healthcare, their response is that they want to help people. They did not want to spend hours in front of a computer clicking boxes. This time-consuming task of documenting in the medical record, or charting, is dull, repetitive, and sometimes disconcerting. It takes time away from being able to provide care for the patient. Yet documentation in the medical record is truly a vital part of patient care.
Nursing documentation fills a significant portion of the medical record. Nurses need make sure what they are adding is accurate and complies with the guidelines set by their facility and the state board. This principle is the same, even though there are differences to be aware of now that the electronic medical record has become the standard.
Self Quiz
Ask yourself...
- What are your experiences with charting? Have you seen examples of correct charting, as well as incorrect nursing documentation charting practices in your field?
The Who, What, When, Where, Why, and How of Nursing Documentation
Who
There are approximately 2.9 million working RNs in the United states, with about 1.6 million working in hospitals (1). Nurses on a med-surg unit typically spend about one-third of their total working hours documenting (2). Considering a nurse on a med-surg floor spends about 2.5 hours per shift charting, that roughly translates into 7 billion hours spent charting nursing documentation each year. And that is only for the nurses!
Every discipline of the healthcare team contributes to the patient’s medical record. These different clinicians may not have the opportunity to report off to one another, and they must refer to the medical record to gather the information they need in order to care for the patient. Even kitchen staff responsible for preparing meals for patients must be able to see the dietary order for the patient. The following are a few examples of the clinicians who contribute to or review the patient’s medical record:
- Medical Team: physicians, nurse practitioners, physician assistants, surgeons, specialists, residents
- Nurses and LPNs
- Medical Assistants, CNAs, patient care assistants or technicians
- Specialty technicians: radiology, anesthesia
- Therapists: physical, speech, occupational, respiratory
- Pharmacists
- Dieticians
- Case managers or social workers
- Coding and billing specialists
- Researchers
What
The primary purpose of the medical record is to communicate data about the patient and care provided between different members of the healthcare team. The bulk of the medical record is a collection of assessment data obtained from the patient. Details concerning assessments and results from lab tests or radiology comprise a large portion of the data. Assessment data is usually collected on a flow sheet system. Progress notes are written by the medical team or therapists and help to guide the intended plan of care for the patient. This is considered narrative charting. The medical record also includes orders for prescribed medications and treatments from the medical team. The following are typical components found in a patient’s medical record.
- Patient demographics: name, age, gender, contact information, language, and insurance information
- Past medical history: surgeries, chronic conditions, family history, allergies, and home prescriptions
- History and Physical (H&P): this can contain information about admitting diagnosis or chief complaint and narrative of the story leading to admission
- Flowsheet of assessment data: vital signs, head-to-toe assessment, intake and output record
- Laboratory test results
- Diagnostic test results: from radiology or procedures
- Clinical notes: progress notes from the medical team, procedure notes, notes from consulting clinicians, education provided, and discharge planning
- Treatment orders
- Medication Administration Record (MAR)
When
The medical record should document every interaction the patient had with a member of the healthcare team. An encounter is created upon admission and everything occurring during a particular admission becomes part of the medical record. Phone calls made to patients and/or families may also become a part of the medical record.
Where
Medical records are stored in various ways depending on their format and the facility. Paper records from small outpatient offices may be kept onsite. Records are now largely kept electronically. This is referred to as the electronic medical record (EMR) or electronic health record (EHR) and consists of Protected Health Information (PHI). They will be stored on a secure server, typically only accessible by authorized personnel.
Why
The medical record is essential to nursing documentation for several reasons. The primary reason for the medical record is that it allows members of the healthcare team the ability to review and analyze data in order to deliver appropriate care. It allows clinicians to keep track of all the care that has already been completed for the patient. It also provides the patient with a record of the treatment they received for as part of their lifetime medical history. The medical record is used for coding and creating a bill for the services the patient received. Medical records may also be used for reviewing processes and research purposes. Ultimately, it is also a legal document and may be used in a court of law as applicable.
How
Medical records are in the final stages of evolution from a paper chart to an electronic medical record system (EMR). By 2017, 96% of acute care hospitals and over 80% of physician offices possessed certified health IT (3). This migration of medical records from paper to electronic format was made possible with advances in technology in the last 30 years. The EMR allows members of the healthcare team to access the medical record instantaneously and improves continuity of care. Utilization of the EMR ultimately reduces costs in healthcare (4) and increases efficiency.
While EMR does have some drawbacks, the benefits that it provides are substantial enough that the government has encouraged its adaptation. The Health Information Technology for Economic and Clinical Health (HITECH) Act was enacted in 2009. This program provided tens of billions of dollars in financial incentives for healthcare facilities to adopt an EMR system (5,6).
Self Quiz
Ask yourself...
- Make your own reference chart of the Who, What, When, Why, and How of nursing documentation.
Privacy and Security in Nursing Documentation
Since 1996, HIPAA, The Healthcare Information Portability and Accountability Act, has been the governing legislation that provides for the privacy protection of medical records. Compliance with HIPAA mandates that anyone who interacts with patients receives training that will ensure that they will maintain privacy for the patient. Part of the HIPAA legislation also allows the patient to request their medical records.
The patient also has the right to request to amend their medical record. Patient permission must be given prior to a third party’s access to their medical record (7). HIPAA legislation was introduced at the advent of EMR technology. A provision of HIPAA provided a framework to ensure privacy of electronic health records (8). However, breaches in security by hackers or cyberterrorists remains a potential threat.
Benefits of the EMR
- Immediate data accessibility and communication of patient status
- Clinicians can view records remotely, analyze the findings, and place orders immediately for faster patient treatment.
- Multiple clinicians can view the chart at one time.
- Records can be viewed easily from previous admissions and/or outpatients visits easily.
- Records can be instantly shared between facilities (in instances of shared systems).
- Reduction in errors
- Errors due to misinterpretation of handwriting in nursing documentation are eliminated.
- Allows for increased safety checks. The EMR can be set to flag missing components of information, tasks that were not yet completed or are overdue, recognize duplicates, and present warnings if documentation has not yet been validated or “signed.”
- Scanning medications is possible with EMR systems to reduce the risk of medication administration errors.
- Assists with appropriate billing by capturing charges of services provided to the patient.
- The EMR can provide reminders for necessity of certain preventative health screenings or vaccines.
- Automatic “signature” of data is completed simply by the user logging in with a unique ID and password. All entries are date and time stamped. If a correction is made, the original data can be accessed.
- Accessing patient EMR is tracked and can be audited to protect patient privacy from unnecessary viewing.
Downsides of the EMR
It is expensive to convert records system to an electronic system:
- The initial cost of the EMR software is very expensive
- More work hours must be paid for staff training and coverage of patients during initial implementation of the program
- Maintaining appropriate encryption and cybersecurity technology against viruses and hacking are also a costly component
Computer systems can be temporarily inaccessible, for example when updates and reboots are required. Paper charting is still necessary in the interim.
Template charting has limitations (9). Templates for nursing documentation may not exist for a specific problem and does not accurately reflect the patient’s condition. Atypical patients may have multiple problems or extensive interventions that must be documented in detail.
Templates may also encourage cloned or copied documentation. It creates unnecessary redundancy and at times inaccurate information in the EHR. Some EHR systems are designed to facilitate cloning with such popular features as:
- “Make me the author” to assume the content of another person’s entry
- “Demo recall” of “Duplicate Results” to copy forward vital signs or assessment data
- “Smart phrases” pulls in specific identical data elements
Automated insertion of previous or outdated information through EHR tools, when not modified to be patient-specific and pertinent to the visit, may raise significant quality of care and compliance concerns.
Self Quiz
Ask yourself...
- Create a T-chart of the benefits versus downsides to EMR.
The Legal Requirements
If it wasn’t documented, it wasn’t done. Every healthcare practitioner has had this mantra ingrained in them from the very beginning of their career. Nurses are trained to document defensively, that is, if they are taught at all.
In a 2014 study, only 20% of new graduate nurses had received electronic medical record training as a part of their nursing school curriculum (6). It is not uncommon for clinicians to have the tendency to view the medical record as a defense tool against potential legal problems, rather than its more significant role as a communication tool for patient care.
Regardless, accurate and complete documentation is essential. Your career, and more importantly, patient care, depends on it.
Self Quiz
Ask yourself...
- Did you receive proper training on documentation in your nursing program?
- How can programs be improved to better prepare nurses?
When Nursing Documentation Becomes Your Defense
In the dreaded event of a legal problem, medical records will be scrutinized to every detail. It is usually the primary source of evidence for the case. A malpractice lawsuit requires four elements to be proven (10):
- That a medical professional assumed a duty to provide care for the patient.
- The clinician failed to provide appropriate care within their scope of practice for the patient.
- The failure in appropriate care caused an injury to the patient.
- The injury resulted in damage to the patient.
Potential legal problems that may arise include the following (11):
- Administrative liability – Professional licensure discipline and/or discharge (firing) from position.
- Civil Liability – Malpractice lawsuit, failure to provide necessary care.
- Criminal liability – Misdemeanor or felony charges for cases of gross negligence.
The Cost
Fortunately, medical malpractice claims have begun to drop since 2001. In 2004, the medical practitioners involved who were known as the defendants won the case 83% of the time. The legal fees can still amount to $18,000 if the case is dropped, to as much as $93,000 even when the case is won (12,13).
In 2018, there were 8,718 malpractice cases that resulted in payments to injured patients (14). Of those events, 310 reports of malpractice suits that resulted in payments related to nursing care.
However, 180 of those, about 60% of those had payments to the injured patient that were over $50,000 (14). However, there were nearly 15,000 adverse action reports filed against nurses, which was more than the number combined filed against physicians, NPs, and PAs combined.
The majority of medical malpractice cases primarily target the physician and the facility. However, anyone who made an entry into the patient’s medical record may be required to participate in legal proceedings.
Most common malpractice claims against nurses include failure to (15):
- Follow standards of care
- Follow safety protocols
- Perform procedures according to guidelines
- Use equipment properly
Use or operate equipment within the manufacture’s details
- Failure to correctly document
- Communication with the provider
- The care you completed
- Follow assess and monitor
- Report a change in status of the physician
- Assess a patient with change in status
- Communicate pertinent data
- Provide appropriate discharge education and information
- Communicate properly and completely between shifts
Self Quiz
Ask yourself...
- Think about the last difficult shift you had. Did you properly complete nursing documentation?
- How would you prioritize documentation differently after reading this module?
What is Required for Nursing Documentation?
Necessary medical record nursing documentation can vary significantly depending on the care area. For example, the documentation a circulating nurse in the operating room completes will be very different from what is documented on an emergency room patient. While the basic principles of documentation stay constant, the nurse needs to be familiar with the documentation requirements for that area based on requirements of the state board of nursing, the facility, and the unit.
There are standard requirements for medical record documentation that are applicable in all patient care settings, and in both paper and EMR systems. These standards include the following (16):
- Accurate: Clinicians must be careful to proofread documentation to make sure it is free from errors. A small typo can have serious repercussions, as it is more likely to be misinterpreted by others.
- Relevant, concise, organized and complete: It is important to keep the information concise and relevant so that other care providers can quickly find the pertinent information that they need. Assessment data should be entered in a systematic way. Complete documentation ensures all of the unit policies for documentation are addressed.
- Free of bias: Clinicians should only include information that is pertinent to the care of the patient and remain free from personal bias. Direct quotations within the proper context should be utilized with proper context.
- Factual: Clinicians should not exaggerate or minimize findings. Charting is to be completed after completing a task, not before. Do not speculate data. Observations need to include exact times and measurements. Avoid approximations. Make sure to chart on the correct patient.
- Timely: What occurred during the shift should be documented during the shift. Documentation should be done as soon as possible after completing tasks. If something needs to be added in after the shift was completed, it should be denoted as a late entry with a reason as to why. Your facility likely has strict requirements regarding late entries.
- Legible/decipherable and clearly written: Paper documentation must be clearly legible. Writing must clearly convey meaning.
- Standardized: Clinicians must use appropriate medical terminology and approved acronyms and abbreviations.
- Labeled and Auditable: Paper documentation must be signed with credentials and must include date and time of the entry. When charting in the EMR, all entries and corrections are recorded and time stamped. Password sharing or having another clinician assist in documenting under incorrect username is fraudulent.
Self Quiz
Ask yourself...
- Do you currently incorporate all of the above principles in your documentation?
- If not, how can you change your practice to improve your documentation?
Examples of Effective and Ineffective Charting
The following will show some examples of these principles in action. These are based on the scenario of a patient admitted in the Emergency Department for chest pain.
| Example of Effective Documentation | Example of Ineffective Documentation | |
| Accuracy | Patient stated she took 800mg of Tylenol at 4pm, an hour after she began to feel chest pain. | Patient reports she took pain med for chest pain. |
| Relevant | Patient stated she has never experienced chest pain prior to this event, and does not have a history of cardiac problems. | Patient was a competitive athlete 20 years ago and used to be in great shape. Patient thinks she is still pretty healthy. |
| Concise | Vital signs taken, telemetry monitor applied, lab samples collected and PIV started per the chest pain protocol. | Patient was triaged and immediately brought to exam room. In accordance with the chest pain protocol, vital signs were taken first. Then the patient had a telemetry monitor applied. Next, the patient had blood samples drawn through the inserted PIV catheter. |
| Organized |
Patient reports no allergies Prescriptions include hormone replacement therapy Past medical history includes hysterectomy and foot surgery from a few years ago Patient family history includes cardiovascular disease on her father’s side of the family Patient denies smoking, illicit drug use, but does drink 3 times a week Patient reports feeling fine until 1 hour after lunch when chest pain began. |
Patient was feeling fine until one hour after lunch, when she started to feel chest pain. Patient has no history of cardiac problems. However there is family history of cardiovascular disease on the father’s side. Patient had a hysterectomy and foot surgery a few years ago. Patient denies smoking and illicit drug use. Patient does take hormone replacement therapy prescription. Patient does not have any allergies. Patient reports drinking alcohol x3/week. |
| Complete | Patient complaining of 8/10 chest pain, described as “stabbing.” Pain has been experiencing this pain for three hours. She has taken Tylenol, but nothing is able to alleviate the pain. | Patient is complaining of chest pain. |
| Free of Bias | Education provided per chest pain protocol. Patient was instructed to call 911 immediately if experiencing chest pain in the future. Patient verbalized understanding. | Patient was given needed education about chest pain since she clearly didn’t understand that chest pain cannot wait 3 hours and she needs to call 911 right away because she can die of a heart attack. |
| Factual | Patient reports last meal was around 1300 which consisted of spicy foods. Her chest pain onset was 30 minutes after. She waited an additional three hours before seeking emergency care. | Patient presented to ER after lunch. |
| Legible/Decipherable | Patient was instructed to call for assistance with ambulation and how to utilize call light. | Patient cannot safe walk by she self. Call light assistance. Bathroom walk with me. |
| Standardized | Morphine Sulphate 2mg IV push, once PRN for 8/10 pain per chest pain protocol. | MSO4 2.0 mg, IV push, x1. |
| Timely | Documentation is completed in real-time, all documentation completed before transferring patient to telemetry. | Nurse documents three days later due to high volume of patients. |
Self Quiz
Ask yourself...
- How can you ensure that your charting is free of bias?
Common Documentation Errors
- Falsification of a record. This can happen when charting an action isn't completed in a timely manner, or from charting information before that action was completed.
- Fraudulent charting is the act of knowingly making a false record. Criminal charges of forgery can result if the misrepresentation is done for personal gain. An example of this would be a nurse documenting at administration of a controlled substance but instead was diverting the medication.
- Inappropriate use of cloning features. Information “copied and pasted” from a different patient’s record or that is completed by another provider. Data copied from previous shift assessments that isn’t updated to reflect current status is also a false record (9).
- Fail to document communication. Notification of the medical team of a change in patient status or critical lab values should always be included. Clarification or confirmation of orders should also be documented (17). Include notification of other providers who assisted with patient are. This includes failure to document transfer of care to another nurse.
- Failing to document a reason why something isn’t done. If a patient doesn’t receive a prescribed medication, the reason why the medication isn’t given needs to be described. If you communicate with the provider, this should also be included.
- If you could alter your documentation, how would you better document in this situation?
- Have you ever failed to document or failed to document a critical portion of care?
Self Quiz
Ask yourself...
Conclusion
Including all of the necessary information into each patient’s medical record can be a daunting task. The nurse must make sure that they have included all of the relevant and accurate information that is required by their facility guidelines. It must usually be done in a loud environment and is frequently interrupted by actually having to provide care to the patients.
It is not only a tedious chore, but it also tends to cause a lot of apprehension. There is usually a worry of “did I chart enough?” or “did I chart everything I needed to?” This is due to the defensive practices and attitudes healthcare workers have adapted to protect against malpractice lawsuits. In this way, charting is similar to paying taxes. No one likes it, but it still has to be done.
Perhaps a way to develop a healthy perspective toward charting is to change the focus to its original purpose: to communicate care about the patient. The purpose of charting is to relay to the other healthcare team members what is going on with the patient. With this objective in mind, the nurse will inevitably cover all the necessary details and it may also be a bit more satisfying to know that even though they are in front of the computer, they are performing and completing important information for the patient.
Nursing Ethics
Introduction
Ethics is an important aspect of all professions, but in this case, we are going to touch on its role in nursing. From the beginning, Florence Nightingale was a strong advocate and initiated nursing ethics and morals. For the 21st consecutive year, nursing has been ranked number one by the Gallup Poll as the most honest and ethical profession (1). This designation creates a larger responsibility to understand the American Nurses Association (ANA) Code of Ethics and how to apply it to practice.
History
Did nursing exist before Nightingale? Yes, but not in an organized fashion, as the formalization of an ethical model began in the mid-1800s with Nightingale. Before she developed a formal training program, nursing was thought to be disreputable, and many people providing caregiving services were prostitutes. Nightingale was the first to instill morals and ethics into education and practice. In 1889, the Trained Nurse and Hospital Review journal was published, including a six-part series on ethics (3, 12).
Following, in 1893, the Nightingale Pledge was written by Listra Gretter to be used at the Farrand Training School for Nurses in Detroit, Michigan (4).
The Pledge is as follows:
"I solemnly pledge myself before God and in the presence of this assembly, to pass my life in purity and to practice my profession faithfully. I will abstain from whatever is deleterious and mischievous and will not take or knowingly administer any harmful drug. I will do all in my power to maintain and elevate the standard of my profession and will hold in confidence all personal matters committed to my keeping and all family affairs coming to my knowledge in the practice of my calling. With loyalty will I endeavor to aid the physician in his work and devote myself to the welfare of those committed to my care" (4).
The Pledge was written 130 years ago; the changes and challenges in nursing over these years are immeasurable.
Nursing Ethics, Principles, and Values
Although nothing had yet been formalized, the idea of ethics in nursing began to spread during the early 1900s. The ANA developed the first Code of Ethics in 1950 and it was revised in 2015. The Nursing Code of Ethics was written to provide guidance for the practice of nursing and to ensure that the highest standard of ethical practice is maintained (11). It was determined the Code of Ethics was necessary for nurses to maintain professional integrity, provide safe and competent care, and promote trust and confidence in the nursing profession (11).
Because nurses provide care for vulnerable people the Code of Ethics also assists in ensuring that safe, competent, and compassionate care is delivered (11).
The principles of the Code of Ethics are based on the guidelines established by the ANA and provide a framework for nursing practice.
There are seven ethical principles (5):
- Autonomy
- Beneficence
- Nonmaleficence
- Veracity
- Confidentiality
- Justice
- Fidelity
Autonomy
This can be as simple as listening to a patient's rights for self-determination, including informed consent and patient choices. How this is viewed depends on the situation (5). It is important to note that in cases of endangering or harming others, for example, through communicable diseases or acts of violence, people lose this basic right (5).
Beneficence
This term refers to doing good and is part of the Nightingale Pledge and the Hippocratic Oath. Showing acts of kindness and facilitating well-being are great examples. However, it is important to understand that we as nurses may think that we know what is best for our patients, but it is never a guarantee that they will agree with us; this is referred to as paternalism (5).
Nonmaleficence
This term almost directly translates to ‘do no harm,’ and can be part of confidentiality or other acts of care that can involve possible negligence. Additionally, it is used in end-of-life situations and decisions of care for terminally or critically ill patients (5).
Veracity
This term requires that you be truthful, accurate, and loyal to not only your patients and their families, but your co-workers as well. Are we telling our patients the truth? Are we holding back information about their conditions? Things to think about include pain medication and dosages (5).
Confidentiality
This ethical principle directs the nurse not to disclose private or sensitive information. Codes of Nursing and Codes of Ethics mandate that nurses maintain confidentiality of patient information. Nurses must keep information confidential, sharing only that which is necessary for patient care (5). Confidential is the only aspect of patient care mentioned in the Nightingale Pledge (5).
Justice
This includes the principle that covers normative aspects that are often discussed in terms of solidarity and reciprocity. Fair distribution of resources and care is an important aspect of this principle (5).
Fidelity
This is the basic principle of keeping your word and can be included in providing safe, quality care (5). If you tell a patient that you will be back to check on their pain level, and you do check back, that is fidelity – you have kept your promise.
When examining nursing ethics, one must consider that the profession has three entry levels: Diploma, Associate’s, and Baccalaureate degrees. This can affect what each nurse learns about, including values and ethics as well their real-life application (5).
Foundations of Nursing Ethics
Nightingale was the first to teach ethics in nursing and set strict codes for those under her supervision; today, the ANA Code of Ethics serves as a concise statement of ethical obligations and duties of every person who enters the profession.
The first three provisions of the ANA Code of Ethics describe the most fundamental values and commitments a nurse must make. The following three include boundaries of duty and loyalty, and the last three demonstrate aspects of duties beyond individual patient encounters (5,11).
Values are important as they remind us as individuals that we all have morals. Being aware of personal values and how our values influence how we relate to others personally and professionally is very important. Values are ideals, customs, beliefs, conduct qualities, and goals. Values are learned in unconscious and conscious ways and become part of who a person is. Values also provide meaning and direction to life. Moral values are the principles and standards that guide us as individuals and assist us in determining what is right and wrong (5.)
Accountability is your responsibility for judgment and actions. To whom are you accountable? Examples include yourself, your family, colleagues, your employer, your patient, and the nursing board. One must take responsibility for their actions (5).
The following are components of accountability:
- Obligation: a duty that usually comes with consequences.
- Willingness: accepted by choice or without reluctance.
- Intent: the purpose that accompanies the plan.
- Ownership: having power or control over something.
- Commitment: a feeling of being emotionally compelled
(5)

Self Quiz
Ask yourself...
- When did ethics begin to develop in nursing?
- How do you define ethics?
- What are the six principles of ethics?
- How do you view patient autonomy?
- Do you think the different entry levels for nursing make a difference in ethics?
- Identify your values.
- Define accountability.
- Identify the components of accountability.
The International Council of Nurses Worldview
Worldview is inclusive of ethical and moral discussions, as well as dilemmas for nurses around the world and primarily focuses on four elements: people, practice, profession, and co-workers (6). The International Council of Nurses (ICN) is more directed toward Worldview. Not all are included in the ANA Code of Ethics.
An interesting factor to note is that the ICN Worldview focuses on co-worker relationships: "Nurse bullying occurs in almost all care settings and units, from the patient floor to the executive suite. 60% of nurse managers, directors, and executives in one 2018 study said they experienced bullying in the workplace, and 26% considered the bullying "severe" (7).
Workplace intimidation is any intimidating or disruptive behavior that interferes with effective healthcare communication and threatens patient safety and is categorized as horizontal or relational aggression. Improving how management addresses such issues in nursing may be critical not only for staff turnover but also for patient outcomes (7).
There is some reluctance to specify the sorts of behavior that will not be tolerated, but effective anti-bullying practices must include a statement of exactly what constitutes bullying. From an ethical perspective, the acceptance of nurses who “eat their young” should no longer be tolerated.
Self Quiz
Ask yourself...
- Define the ANA Code of Ethics.
- Evaluate and review horizontal aggression in the workplace. Have you experienced it?
- How do your culture and background affect your practice?
- What workplace behaviors should not be tolerated?
Application
As patient advocates, nurses work as part of an interdisciplinary team to provide patient care. Nursing ethics have kept pace with the advancement of the profession to include a patient-centered focus rather than a physician-centered focus. Due to its focus on providing care, nursing ethics are often different than medical ethics; and we need to understand the differences.
As we discuss application, one must take into consideration the workforce of nurses today. In many facilities, nursing staff may encompass at least three and maybe even four generations. This also applies to our patients.
Those generations are identified as follows:
- Traditionalists or Silent Generations (1922- 1946):
- They have respect for authority, are hardworking, and are sacrificial for their work. Many have delayed retirement (8)
- Baby Boomers (1946- 1964):
- Possess a belief that workers must pay their dues, are workaholics, and typically rely on traditional learning styles (8).
- Generation X (1965-1977):
- Independent, a skeptic of authority, and self-reliant (8).
- Generation Y (1978-1991):
- Team-oriented, tech-savvy, entrepreneurial, and has a desire to receive feedback (8).
- Generation Z (1992- 2012):
- Tech savvy understands the power of text and social media. (8)
- Tech savvy understands the power of text and social media. (8)
Regardless of what generation you fall into, it is important to understand and respect the different personalities and learning styles of everyone.
A prime example of the generational learning styles differing and potential issues that may arise is the usage of electronic health/medical records (EMR) and various other health information technologies that are often incorporated into daily nursing practice.
Nurses that come from older generations may struggle with these more, as they have experienced its transition and had to adapt (8).
As the prevalence of social networking platforms continues to rise, nurses need to understand the ethics of social media. Issues of privacy confidentiality and anonymity are ethical concerns when mixing personal and professional information on a social media platform. It is also important to note that most healthcare facilities have strict policies regarding social media.
End-of-Life
End-of-life issues are filled with nursing ethics and dilemmas. If the advanced directive is not clear, family issues and other complications trigger many of the ethical principles. Self-determination (the right to stop or refuse treatment) is complicated, the patient may not always have their wishes on paper, and often, families do not want to let go.
Nurses are the backbone of allowing the patient's wishes to be known. Nurses must know that they can request an ethics committee review for their patients if they feel their wishes are being violated (10).
Additionally, physician-assisted suicide can be an extraordinarily complex issue. For both the Hippocratic Oath and the Nightingale Pledge, there are ethical issues. Currently, the following states have made physician-assisted suicide legal: California, Colorado, Hawaii, Maine, New Jersey, Oregon, Montana, The District of Columbia, and Washington (9). With the ever-expanding ability to both prolong and end life; nurses must be cognizant and prepared for all repercussions associated with life-and-death situations (10).
With recent societal and technological advancements in science and medicine, choices involving both life and death seem to become more complicated. As a result of this worldwide controversy in healthcare, many nurses nationwide are now forced to deal with this ethical dilemma head-on (10). There are and will be many debates as to the ethical issues involved in physician-assisted suicide and something on the forefront for nursing to consider.

Self Quiz
Ask yourself...
- Evaluate your work environment and the differences in generations.
- Think about what ethical dilemmas you face daily.
- Evaluate and review horizontal aggression in the workplace. Have you experienced it?
- How do your culture and background affect your practice?
- What workplace behaviors should not be tolerated?
The ANA Code of Ethics
The ANA Code of Ethics serves to guide nurses in maintaining ethical standards and in ethical decision-making. Additionally, it outlines the obligations nurses must have for their patients and the nursing profession. The provisions focus on the following as stated by Lockwood (11):
- Respect for human dignity: The nurse must show respect for the individual and consider multiple factors (belief systems, gender/sexual identification, values, right to self-determination, and support systems) when planning and providing care. The nurse ensures patients are fully informed and prepared to make decisions about their healthcare and to carry out advance healthcare planning.
- Commitment to patients: The nurse must always remember that the primary responsibility is to the patient and help resolve conflicts between the patient and others and avoid conflicts of interest or breach of professional boundaries.
- Protection of patients’ rights: The nurse must be aware of legal and moral responsibilities related to the patients’ rights to privacy and confidentiality (as outlined by HIPAA regulations) and research participation.
- Accountability: The nurse bears primary responsibility for the care of the patient and must practice according to the Code of Ethics and the state nurse practice act and any regulations or standards of care that apply to nursing and healthcare.
- Professional growth: The nurse must strive always to promote health, safety and wellbeing of self and others. The nurse must, in all circumstances, maintain personal integrity and report violations of moral standards. The nurse has a right to refuse to participate in actions or decisions that are morally objectionable but cannot do so if this refusal is based on personal biases against others rather than legitimate moral concerns.
- Improvement of healthcare environment: The nurse must recognize that some virtues are expected of nurses, including those associated with wisdom, honesty, and caring for others, and that the nurse has ethical obligations toward others. The nurse is also responsible for creating and sustaining a moral working environment.
- Advancement of the profession: The nurse must contribute to the profession by practicing within accepted standards, engaging in scholarly activities, and carrying out or applying research while ensuring the rights of the patients are protected.
- Health promotion efforts: The nurse recognizes that health is a universal right for all individuals and collaborates with others to improve general health and reduce disparities. The nurse remains sensitive to cultural diversity and acts against human rights violations, such as genocide, and other situations that may endanger human rights and access to care.
- Participation in goals of the profession: The nurse must promote and share the values of the profession and take action to ensure that social justice is central to the profession of nursing and healthcare.

Conclusion
In conclusion, nurses face ethical dilemmas in practice almost every day, which is why it is so valuable for nurses to understand the philosophy of nursing ethics and its application in practice. The ANA Code of Ethics is a valuable guideline for nurses and should be followed to ensure that all nurses practice ethically.
Infection Control and Barrier Precautions
Healthcare professionals have the responsibility to adhere to scientifically accepted principles and practices of infection control in all healthcare settings and to oversee and monitor those medical and ancillary personnel for whom the professional is responsible.
Introduction
The healthcare industry is held accountable to keep patients safe with nursing having a pivotal role. Nurses must adhere to the guidelines set in place to ensure that care is aimed at infection prevention for both healthcare workers and patients. Modes and mechanisms of transmission of pathogenic organisms in the healthcare setting and strategies for prevention control are necessary. As is the use of engineering and work practice controls to reduce the opportunity for patient and healthcare worker exposure to potentially infectious material in all healthcare settings. Creation and maintenance of a safe environment for patient care in all healthcare settings through application of infection control principles and practices for cleaning, disinfecting, and sterilization is extremely important.
Self Quiz
Ask yourself...
- Why is it important to adhere to infection control guidelines?
Element I
Healthcare professionals have the responsibility to adhere to scientifically accepted principles and practices of infection control in all healthcare settings and to oversee and monitor those medical and ancillary personnel for whom the professional is responsible.
Element I Objectives
At the conclusion of course work or training on this element, the learner will be able to:
- Recognize the benefit to patients and healthcare workers of adhering to scientifically accepted principles and practices of infection prevention and control.
- Recognize the professional’s responsibility to adhere to scientifically accepted infection prevention and control practices in all healthcare settings and the consequences of failing to comply.
- Recognize the professional’s responsibility to monitor infection prevention and control practices of those medical and ancillary personnel for whom they are responsible and intervene as necessary to assure compliance and safety.
The healthcare industry is held accountable to keeping patients safe, with nursing having a pivotal role. Nurses must adhere to the guidelines set in place to ensure that care is aimed at infection prevention for both healthcare workers and patients.
Statements from Relevant Professional and National Organizations
As the largest healthcare workforce in the nation, nurses are able to positively affect the rates of infection at the bedside. The Center for Disease Control asserts the minimum accepted practice of preventing infection is with the use of Standard Precautions, with the number one action in prevention being proper hand washing (3).
The American Nurses Association refers to similar basic tenets of infection prevention: thorough hand washing, staying home when ill, ensuring vaccinations are complete and up to date, using appropriate personal protective equipment, and covering face when coughing or sneezing (4).
In 2017, the CDC, ANA, and 20 other professional nursing organizations collaborated to create the Nursing Infection Control Education (NICE) Network. This team effort is aimed at introducing clear obligations and competencies for nursing and all healthcare providers to stop the spread of microorganisms within health care systems. Within these cores is the responsibility of nursing as leaders within healthcare, “To be successful, infection prevention programs require visible and tangible support from all levels of the healthcare facility’s leadership” (5).
Self Quiz
Ask yourself...
- Which organizations have collaborated to put guidelines in place?
- What does this say about the importance of infection control?
Implications of Professional Conduct Standards
As healthcare professionals that participate in and supervise care of patients, nurses are responsible for being knowledgeable of the guidelines set by State and federal bodies. Several of these will be touched on throughout this course.
The responsibility also applies to delegated activities. The nurse must ensure that the five rights of delegation are considered when assigning a task to unlicensed assistive personnel and that appropriate infection control policies and protocols are being followed appropriately. Always refer to facility policies and procedures to avoid potentially adverse outcomes.
Failure to follow the accepted standards of infection prevention and control may have serious health consequences for patients, as well as healthcare workers. Hospital acquired infections (HAI) have improved by 16% from 2011 to 2015; however, the CDC reports that in 2015 there were still approximately 687,000 HAIs with 72,000 resulting in death (6).
In cases of nurses observing incompetent care or unprofessional conduct in relation to infection control standards, the chain of command should first be utilized. Taking consideration into the type of misconduct, the improper infection control infraction should be addressed according to facility policy. Charge nurses and managers would be wise to first address the issue with the nurse involved to gather information and address any education deficits.
In cases where clear misconduct is evident, the National Council of State Boards of Nursing advises, “A nurse’s practice and behavior is expected to be safe, competent, ethical and in compliance with applicable laws and rules. Any person who has knowledge of conduct by a licensed nurse that may violate a nursing law or rule, or related state or federal law may report the alleged violation to the board of nursing where the conduct occurred” (7).
Consequences of failing to follow accepted standards of infection prevention and control may result in a complaint investigation from your various state of employments Professional Misconduct Enforcement Systems. Upon investigation, penalties include, but are not limited to, reprimand and censure, fines totaling thousands of dollars per violation, and probationary terms.
Severe misconduct may result in the loss or revocation of a nursing license. As well, in cases where the neglect to follow appropriate conduct has resulted in harm to a patient or co-worker, there is potential for professional liability through a malpractice suit brought against the nurse.
Methods of Compliance
Nurses are responsible for being knowledgeable of the licensure renewal requirements and targeted education in their state of practice. Refer to your specific state’s Board of Nursing for further guidance beyond the above-mentioned licensing requirements.
Education of infection control best practice, complying with state requirements, and following the facility practices and policies will provide the best protection for self, patients, and staff in preventing and controlling infection during patient care.
Self Quiz
Ask yourself...
- Can you list some requirements in your specific state, regarding infection control?
Element II
Modes and mechanisms of transmission of pathogenic organisms in the healthcare setting and strategies for prevention control.
Element II Objectives
Upon completion of course work or training on this element, the learner will be able to:
- Describe how pathogenic organisms are spread in healthcare settings
- Identify the factors which influence the outcome of an exposure to pathogenic organisms in healthcare settings
- List strategies for preventing transmission of pathogenic organisms
- Describe how infection control concepts are applied in professional practice
Definitions
Pathogen or infectious agent: A biological, physical, or chemical agent capable of causing disease. Biological agents may be bacteria, viruses, fungi, protozoa, helminths, or prions.
Portal of entry: The means by which an infectious agent enters the susceptible host.
Portal of exit: The path by which an infectious agent leaves the reservoir.
Reservoir: Place in which an infectious agent can survive but may or may not multiply or cause disease. Healthcare workers may be a reservoir for several nosocomial organisms spread in healthcare settings.
Standard precautions: A group of infection prevention and control measures that combine the major features of Universal Precautions and Body Substance Isolation and are based on the principle that all blood, body fluids, secretions, excretions except sweat, non-intact skin, and mucous membranes may contain transmissible infectious agents.
Susceptible host: A person or animal not possessing sufficient resistance to a particular infectious agent to prevent contracting infection or disease when exposed to the agent.
Transmission: Any mechanism by which a pathogen is spread by a source or reservoir to a person.
Common vehicle: Contaminated material, product, or substance that serves as a means of transmission of an infectious agent from a reservoir to one or more susceptible hosts through a suitable portal of entry.
Self Quiz
Ask yourself...
- In what context have you used this terminology in your facility?
Overview of Components of the Infectious Disease Process
The infectious disease process follows a particular sequence of events that is commonly described as the “The Chain of Infection.” Nurses must have a solid understanding of this process in order to identify points in the chain where the spread of infection may be prevented or halted. The sequence involves six factors: pathogen, reservoir, portal of exit, portal of entry, mode of transmission, and a susceptible host. The cyclical and consistent nature of the chain provides ample opportunities to utilize scientific, evidence-based measures in combating infection spread.
Pathogens within healthcare are widespread and plentiful, putting patients and healthcare workers at particular risk for contamination. The manifestation of symptoms and mode of transmission is varied depending upon the characteristic of the specific infectious agent. Healthcare workers are at a much higher risk for bloodborne pathogens such as human immunodeficiency virus (HIV), hepatitis B virus, and hepatitis C virus. Influenza, methicillin-resistant Staphylococcus aureus (MRSA), and Tuberculosis (TB) also poses a higher risk (1). Due to the immunocompromised systems of patients, these and many other pathogens cause a considerable risk and can result in HAIs such as Central Line-associated Bloodstream Infection (CLABSI), Catheter-associated Urinary Tract Infections (CAUTI), Surgical Site Infection (SSI), and Ventilator-associated Pneumonia (VAP) (1).
Pathogens require a reservoir, which is typically a human or animal host; however, may also be from the environment, such as standing water or a surface. From the reservoir, the pathogen is spread via a mechanism such as body fluid, blood, or secretions. Common sites for contact within patient care include the respiratory, genitourinary, and gastrointestinal tracts, as well as skin/mucous membranes, transplacental, or blood. From here, the mechanism must come into contact with another portal of entry. Transmission may occur through respiratory, genitourinary, and gastrointestinal tracts, skin and/or mucous membranes, transplacental, and parenteral pathways. Some of these sites may have become compromised during patient care due to percutaneous injury, invasive procedures or devices, or surgical incisions.
In order to acquire a pathogen, a mode of transmission must be provided. These can be from contact, transmission via a common vehicle, or vector borne.
Contact with a pathogen may be categorized as direct, indirect, droplet, or airborne. Contact transmission is through direct or indirect contact with a patient or objects that have been in contact with the patient. Pathogens related to this include Clostridium difficile and multi-drug resistant bacteria such as MRSA. Droplet transmission occurs when a pathogen can infect via droplets through the air by talking, sneezing, coughing, or breathing. The pathogen can travel three to six feet from the patient. Airborne transmission occurs when pathogens are 5 micrometers or smaller in size and are capable of being suspended in the air for long periods of time. These types of pathogens include tuberculosis, measles, chickenpox, disseminated herpes zoster, and anthrax (2).
Transmission may also occur through a common vehicle which affects multiple hosts and can come from food, intravenous fluid, medication, biofilms, or equipment that is shared and often leads to widespread outbreaks. Vector borne pathogens are derived from a living vector such as mosquitoes, fleas, or ticks.
The last factor in the chain of infection is a susceptible host with a mode of entry. This is the reason that patients are at a much higher risk for developing secondary infections within the healthcare system.
Factors Influencing the Outcome of Exposures
The human body provides several natural defenses to prevent infection from a pathogen. The most prominent defense is the integumentary system and focus should be on maintaining skin integrity to prevent a mode of entry. Respiratory cilia function to move microbes and debris from airway. Gastric acid is at an optimal pH level that prevents the growth of many pathogens. Bodily secretions provide defense through flushing out and preventing back-flow of potential infectious agent colonization. The normal flora also provides a layer of defense that must take care to not be compromised through use of antibiotics. Probiotics are commonly administered to patients on antibiotics to prevent a secondary infection due to the normal flora being disrupted (3).
Host immunity is the secondary defense that utilizes the hosts own immune system to target invasive pathogens. There are four types of host immunity (all from 3):
- Inflammatory response is pathogen detection by cells in a compromised area that then elicit an immune response that increases blood flow. This inflammatory response provides delivery of phagocytes or white blood cells to the infected site response. The phagocytes are designed to expunge bacteria.
- Cell mediated immunity uses B-cells and T-cells, specialized phagocytes, are cytotoxic cells which target pathogens.
- Humoral immunity is derived from serum antibodies produced by plasma cells.
- Immune memory is the ability of the immune system to recognize previously encountered antigens of pathogens and effectively initiate a targeted response.
Pathogen or Infection Agent Factors
For each type of infectious agent, there are specific factors that determine the risk to the host. Infectivity refers to the number of exposed individuals that become infected. Pathogenicity is the number of infected individuals that develop clinical symptoms and virulence is the mortality rate of those infected. The probability of an infectious agent to cause symptoms depends upon the size of inoculum (amount of exposure), and route and duration of exposure (4).
The environment is another factor that warrants attention in limiting the probability of exposure in the healthcare setting. Fomites are materials, surfaces or objects which are capable of harboring or transmitting pathogens. These can be bedside tables, scrubs, gowns, bedding, faucets, and any other number of items that are in contact with patients and healthcare providers (7).
Equipment is also a common means of spreading infection, especially portable medical equipment that can come into contact with numerous patients in a day. This can include vitals machines, IV pumps, wheelchairs, and computers on wheels, among numerous other care items frequently used. Care must be taken to ensure cleaning in between each patient use. For patient’s in isolation, dedicated equipment for that patient should remain in the room for the duration of stay.
Self Quiz
Ask yourself...
- How can you limit the outcome of exposures as a medical professional?
Methods to Prevent the Spread of Pathogenic Organisms in Healthcare Settings
Standard Precautions
Standard precautions are the minimal amount of caution and procedure applied to typical patient care. According to the CDC, standard precautions are to be used in all patient care areas with critical thinking applied to “. . . common sense practices and personal protective equipment use” (5). The primary of these is proper hand hygiene to be exercised by healthcare providers, patients, and visitors. They will be covered in further detail in this course.
Standard precautions provide guidelines for respiratory hygiene and cough etiquette. The CDC recommends that the mouth and nose be covered with a tissue when coughing or sneezing, with appropriate disposal of the tissue in the nearest waste station. Hand hygiene is to be performed after any contact with any respiratory secretions or contact with potentially contaminated items (5).
As mentioned, healthcare workers are at a higher risk for bloodborne infections due to handling of sharps. Approximately 385,000 needle sticks and sharps injuries are reported by healthcare workers in hospital settings each year (5). Standard precautions can be applied to ensure safe injection practices and will be further covered in Element III.
Certain spinal procedures that access the epidural or subdural space provide a means of transmission for infection such as bacterial meningitis. The CDC states (all from 6):
- Face masks should always be used when injecting material or inserting a catheter into the epidural or subdural space.
- Aseptic technique and other safe injection practices (e.g., using a single-dose vial of medication or contrast solution for only one patient) should always be followed for all spinal injection procedures.
For Patients Infected with Organisms other than Bloodborne Pathogens
Special considerations must be given to patient populations that are infected with organisms other than bloodborne pathogens. During triage of a patient entering a facility, a thorough history should be obtained. This would include exposure to infectious agents, travel to certain countries in the world, and previous infections that are resistant to antibiotics (i.e., MRSA, VRE, or carbapenem-resistant Enterobacteriaceae). Patients that are identified with risk may be placed on the appropriate precautions in an isolation room. Infection prevention and the attending physician should be consulted immediately for further orders and treatment.
Control of Routes of Transmission
Controlling the routes of transmission is a key factor in preventing infection spread. Hand hygiene has been established as providing the primary prevention method. Care must be taken to follow guidelines for proper hand washing including:
- Use antibacterial soap and water when hands are visibly soiled or when a Clostridium difficile infection is known or suspected.
- Hands should be lathered ensuring all surfaces, between fingers, and under nails is covered and scrubbing should last at least 20 seconds.
- Thoroughly rinse soap from hands with running water, pat dry with paper towel, and use paper towel to turn off faucet.
- Hand sanitizer that is at least 60% alcohol based may be used in between soap and water use.
- A dime sized amount of hand sanitizer should be rubbed over surface of hands and fingers, then allowed to air dry.
Barriers to proper hand hygiene include knowledge gaps and availability of appropriate supplies. Training programs to educate healthcare providers on proper hand washing should be accompanied with ongoing assessment and feedback to ensure that compliance is met. Incorporating hand hygiene into the professional development plan of each nurse is also recommended (7). Healthcare facilities should be diligent in ensuring that hand washing stations are located in convenient areas and that hand cleaning product is frequently monitored and refilled (7,8). Signage and educational materials may be posted in high traffic areas and at hand washing stations to encourage use by healthcare providers, patients, and visitors (7).
Nurses and healthcare personnel must be aware of the potential of hand hygiene materials as being a possible source of contamination or cross-contamination. Hand hygiene dispensers are touched frequently with contaminated hands and must be frequently cleaned. Follow manufacturers recommendations for cleaning.
Hand hygiene systems that allow product to be refilled pose a risk of contaminating the contents. If refilling is a requirement, this should be accomplished using aseptic technique as much as possible. Facilities should avoid purchasing this type of product and move to pre-filled dispensing units, if possible (10).
Use of Appropriate Barriers
Appropriate barriers are essential in keeping patients and healthcare providers safe from transmitting or contracting pathogens. The type of PPE chosen depends on certain variables such as the patient care being provided, standard precautions, and transmission-based precautions. The minimal amount of PPE recommended are as follows:
- Contact precautions require gloves and gowns. If bodily secretions may be contacted, a mask and eye protection are required.
- Droplet precautions require a surgical mask.
- Airborne precautions require the wearing of gloves and a gown as well as an approved N95 respirator mask that has been fit tested for the individual wearing. Negative pressure rooms that are able to filter 6 to 12 air exchanges per hour are also recommended (1).
Be mindful that these are the minimal recommendations based solely on the identified transmission status of the patient. Selection of PPE should be made using critical thinking to identify potential risks depending on type of patient care being performed, procedure, behavioral considerations, and other factors that may deviate from the standard.
The following are current recommendations from the CDC for donning and doffing (all from 11).
How to Put On (Don) PPE Gear
More than one donning method may be acceptable. Training and practice using your healthcare facility’s procedure is critical. Below is one example of donning.
- Identify and gather the proper PPE to don. Ensure choice of gown size is correct (based on training).
- Perform hand hygiene using hand sanitizer.
- Put on isolation gown. Tie all the ties on the gown. Assistance may be needed by other healthcare personnel.
Put on NIOSH-approved N95 filtering face-piece respirator or higher (use a facemask if a respirator is not available).
If the respirator has a nosepiece, it should be fitted to the nose with both hands, not bent or tented. Do not pinch the nosepiece with one hand. Respirator/facemask should be extended under chin. Both your mouth and nose should be protected. Do not wear respirator/facemask under your chin or store in scrubs pocket between patients.
-Respirator: Respirator straps should be placed on crown of head (top strap) and base of neck (bottom strap). Perform a user seal check each time you put on the respirator.
-Facemask: Mask ties should be secured on crown of head (top tie) and base of neck (bottom tie). If mask has loops, hook them appropriately around your ears.
5. Put on face shield or goggles.
When wearing an N95 respirator or half face-piece elastomeric respirator, select the proper eye protection to ensure that the respirator does not interfere with the correct positioning of the eye protection, and the eye protection does not affect the fit or seal of the respirator. Face shields provide full face coverage. Goggles also provide excellent protection for eyes, but fogging is common.
6. Put on gloves. Gloves should cover the cuff (wrist) of gown.
7. Healthcare personnel may now enter patient room.
How to Take Off (Doff) PPE Gear
More than one doffing method may be acceptable. Training and practice using your healthcare facility’s procedure is critical. Below is one example of doffing.
- Remove gloves. Ensure glove removal does not cause additional contamination of hands. Gloves can be removed using more than one technique (e.g., glove-in-glove or bird beak).
- Remove gown. Untie all ties (or unsnap all buttons). Some gown ties can be broken rather than untied. Do so in gentle manner, avoiding a forceful movement. Reach up to the shoulders and carefully pull gown down and away from the body. Rolling the gown down is an acceptable approach. Dispose in trash receptacle.
- Healthcare personnel may now exit patient room.
- Perform hand hygiene.
- Remove face shield or goggles. Carefully remove face shield or goggles by grabbing the strap and pulling upwards and away from head. Do not touch the front of face shield or goggles.
- Remove and discard respirator (or face mask if used instead of respirator). Do not touch the front of the respirator or face mask.
-Respirator: Remove the bottom strap by touching only the strap and bring it carefully over the head. Grasp the top strap and bring it carefully over the head, and then pull the respirator away from the face without touching the front of the respirator.
-Face mask: Carefully untie (or unhook from the ears) and pull away from face without touching the front. - The final step is to perform hand hygiene after removing the respirator/face mask and before putting it on again if your workplace is practicing reuse.
Self Quiz
Ask yourself...
- How have barriers changed in your local area since the outbreak of COVID-19?
Appropriate Isolation/Cohorting of Patients with Communicable Diseases
Cohorting patients is a common practice within facilities, especially with limited rooms and an increasing number of patients with MDROs (12). In order to combat these issues, placing patients with the same type of pathogen in one room, when single rooms are not available is an option. The minimal standard for all patients is standard precautions.
The CDC offers guidance for appropriately isolating or cohorting patients based on the type of precaution.
Contact: Patients with a known or suspected pathogen that is transmitted via contact should be placed in a private room, if available. Cohorting can be achieved if the cohorted patients share the same type of pathogen (13).
Droplet: Unless a single patient room is not available, patients in droplet precautions should only be cohorted if neither have an excessive cough or sputum production. The cohorts should be tested to ensure they are infected with the same type of pathogen. Immunocompromised patients are at an increased risk and should not be cohorted. Patients are to be separated at least three feet apart and a privacy curtain should remain drawn between their respective areas. Care providers must don and doff new PPE in between providing care to each respective patient (13).
Airborne: An airborne infection isolation room (AIIR) with negative air pressure that exchanges air at least 6 to 12 changes per hour is required. The door must remain closed except for entry and exit. Cohorting of patients is not recommended except in the case of outbreak or large number of exposed patients (13). In these instances, the CDC recommends the following (13):
- Consult infection control professionals before patient placement to determine the safety of alternative rooms that do not meet engineering requirements for AIIR.
- Place together (cohort) patients who are presumed to have the same infection (based on clinical presentation and diagnosis when known) in areas of the facility that are away from other patients, especially patients who are at increased risk for infection (e.g., immunocompromised patients).
- Use temporary portable solutions (e.g., exhaust fan) to create a negative pressure environment in the converted area of the facility. Discharge air directly to the outside, away from people and air intakes, or direct all the air through HEPA filters before it is introduced to other air spaces.
Host Support and Protection
Vaccinations to preventable disease are highly recommended by numerous health organizations such as the CDC, World Healthcare Organization, and the Office of Disease Prevention and Health Promotion. As state by Healthy People 2020, “. . . infectious diseases remain a major cause of illness, disability, and death. Immunization recommendations in the United States currently target 17 vaccine-preventable diseases across the lifespan” (14). As healthcare providers, nurses are in a position to review the patient’s history for gaps in appropriate vaccination coverage and offer education to the patient. Additionally, healthcare providers hold an ethical responsibility to stay current on vaccinations and prevent transmitting known communicable diseases by receiving an influenza vaccination each year.
Pre- and/or post-prophylaxis may be recommended during certain types of exposures or for patients at an increased risk for infection. This is commonly used for emergent or planned procedures and surgeries that access areas that are at higher risk for becoming a portal of entry, such as the respiratory, gastrointestinal, and genitourinary tracts. Antibiotics may be ordered when it is known that the sterile field has been broken during a procedure or there has been a concern of contamination of a wound or incision site.
In cases of exposure to an infectious pathogen, the decision to treat includes factors such as the type of exposure, patient’s symptoms, time frame since exposure, the health status of the individual exposed, as well of the risks and benefits of the treatment. Pre-prophylaxis may be considered in the prevention of HIV for high-risk individuals.
Typically, after an exposure, the host’s blood is drawn to determine pathogen risk regardless if there is a known pathogen. Post-exposure prophylactics are given within a short time frame from the exposure based on results. The individual that is exposed will have baseline testing for HIV, hepatitis B virus, and hepatitis C viral antibodies. Follow-up testing occurs six weeks, three months, and six months after initial exposure.
Maintaining skin and immune system integrity is of the upmost importance to prevent the transmission of infectious pathogens. Nursing interventions to promote skin and immune system integrity are:
- Perform a thorough skin assessment every shift and with changes in condition
- Accurately document any wounds or incisions
- Use gentle cleansers on skin and pat dry
- Use moisturizers and barrier creams on dry or tender skin
- Prevent pressure ulcer development by turning and repositioning patient every 2 hours
- Maintain aseptic technique during wound care, dressing changes, IV manipulation or blood draws, and catheter care
- Use neutropenic guidelines when providing care to immunocompromised patients
- Encourage adequate nutritional and intake
Environmental Control Measures
The cleaning, disinfection and sterilization of patient care equipment should be performed per the recommendations of the manufacturer. Cleaning should be performed between multiple patient use. For equipment that has been used in an isolation room, a terminal clean must be performed prior to being used in any other patient care. Additional information on this topic will be covered within Element V.
Environmental cleaning personnel must be educated on the appropriate cleaning for all precaution patient environments. The Material Safety Data Sheets for all chemicals are to be available to all healthcare personnel for reference as to the proper use and storage. These should be referred to in order to ensure that the correct cleaning product is effective to terminally clean isolation rooms based on pathogen.
Ventilation should be thoroughly managed and maintained by the environmental operations team. Negative pressure rooms should be consistently monitored, and alarms investigated to ensure proper air exchange. Concerns from nursing regarding ventilation issues should be directed to the environmental team for follow-up.
Regulated medical waste (RMW) within the healthcare system that must follow state guidelines for disposal includes:
- Human pathological waste
- Human blood and blood products
- Needles and syringes (sharps)
- Microbiological materials (cultures and stocks)
- Other infection waste (16)
According to the CDC, “To ensure containment, RMW (except medical waste sharps) is required to be placed in plastic bags and then packaged in single use (e.g., corrugated boxes) or reusable rigid (e.g., plastic) or semi-rigid, leak proof containers before transport. Once packaged, RMW is either transported to a designated secure storage or collection area within the facility for third party pick-up, or to a generator’s on-site treatment facility” (15).
Bodily fluid (urine, vomit, and feces) may be safely disposed of in any utility sink, drain, toilet, or hopper that drains into a septic tank or sanitary sewer system. Healthcare personnel must don appropriate PPE during disposal.
Self Quiz
Ask yourself...
- What are some ways vehicles for infectious matter can be contained?
Element III
Use of engineering and work practice controls to reduce the opportunity for patient and healthcare worker exposure to potentially infectious material in all healthcare settings.
Element III Objectives
Upon completion of course work or training on this element, the learner will be able to:
- Define healthcare-associated disease transmission, engineering controls, safe injection practices, and work practice controls
- Describe specific high-risk practices and procedures that increase the opportunity for healthcare worker and patient exposure to potentially infectious material
- Describe specific measures to prevent transmission of blood-borne pathogens from patient to patient, healthcare worker to patient, and patient to healthcare worker via contaminated injection equipment
- Identify work practice controls designed to eliminate the transmission of blood-borne pathogens during use of sharp instruments (e.g., scalpel blades and their holders (if not disposable), lancets, lancet platforms/pens, puncture devices, needles, syringes, injections)
- Identify where engineering or work practice controls can be utilized to prevent patient exposure to blood-borne pathogens
Definitions
Healthcare-associated infections (HAIs): Infections associated with healthcare delivery in any setting (e.g., hospitals, long-term care facilities, ambulatory settings, home care).
Engineering Controls: Controls (e.g., sharps disposal containers, self-sheathing needles, safer medical devices, such as sharps with engineered sharps injury protections and needleless systems) that isolate or remove the blood-borne pathogens hazard from the workplace.
Injection safety (or safe injection practices): A set of measures taken to perform injections in an optimally safe manner for patients, healthcare personnel, and others. A safe injection does not harm the recipient, does not expose the provider to any avoidable risks and does not result in waste that is dangerous for the community. Injection safety includes practices intended to prevent transmission of blood-borne pathogens between one patient and another, or between a healthcare worker and a patient, and to prevent harms such as needlestick injuries.
Single-use medication vial: A bottle of liquid medication that is given to a patient through a needle and syringe. Single-use vials contain only one dose of medication and should only be used once for one patient, using a new sterile needle and new sterile syringe.
Multi-dose medication vial: bottle of liquid medication that contains more than one dose of medication and is often used by diabetic patients or for vaccinations.
Work Practice Controls: Controls that reduce the likelihood of exposure to blood-borne pathogens by altering the way a task is performed (e.g., prohibiting recapping of needles by a two-handed technique).
Self Quiz
Ask yourself...
- Do you know the measures for injection safety?
High-Risk Practices and Procedures Capable of Causing Healthcare Acquired Infection with Blood-borne Pathogens
Percutaneous exposures are a work hazard within the healthcare industry. There are approximately 5.6 million healthcare workers at risk, with nurses ranking number one. Studies have shown that needlestick injuries occur most frequently within a patient room or the operating room (1).
Exposures can occur through not following safe practices. The following practices in handling contaminated needles and other sharp objects, including blades, can increase the risk for a percutaneous exposure and should be avoided.
- Manipulating contaminated needles and other sharp objects by hand (e.g., removing scalpel blades from holders, removing needles from syringes)
- Delaying or improperly disposing (e.g., leaving contaminated needles or sharp objects on counters/workspaces or disposing in non-puncture-resistant receptacles)
- Recapping contaminated needles and other sharp objects using a two-handed technique
- Performing procedures where there is poor visualization, such as:
- Blind suturing
- Non-dominant hand opposing or next to a sharp
- Performing procedures where bone spicules or metal fragments are produced
Mucous membrane/non-intact skin exposures occur with direct blood or body fluids contact with the eyes, nose, mouth, or other mucous membranes via the following.
- Contact with contaminated hands
- Contact with open skin lesions/dermatitis
- Splashes or sprays of blood or body fluids (e.g., during irrigation or suctioning)
Parenteral exposure is the subcutaneous, intramuscular, or intravenous contact with blood or other body fluid. Injection with infectious material may occur during the following scenerios.
- Administration of parenteral medication
- Sharing of blood monitoring devices (e.g., glucometers, hemoglobinometers, lancets, lancet platforms/pens)
- Infusion of contaminated blood products or fluids
- Safe injection practices and procedures designed to prevent disease transmission from patient to patient and healthcare worker to patient
According to the CDC, unsafe injection practices have resulted in more than 50 outbreaks of infectious disease transmission since 2001. As well, since that time over 150,000 patients were potentially exposed to HIV, hepatitis B virus, and hepatitis C virus solely due to unsafe practice (2). These deviations from best practice have resulted in one or more of the following consequences.
- Transmission of blood-borne viruses, including hepatitis B and C viruses to patients
- Notification of thousands of patients of possible exposure to blood-borne pathogens and recommendation that they be tested for hepatitis C virus, hepatitis B virus, and human immunodeficiency virus (HIV)
- Referral of providers to licensing boards for disciplinary action
- Malpractice suits filed by patients
Pathogens including HCV, HBV, and human immunodeficiency virus (HIV) can be present in sufficient quantities to produce infection in the absence of visible blood.
- Bacteria and other microbes can be present without clouding or other visible evidence of contamination.
- The absence of visible blood or signs of contamination in a used syringe, IV tubing, multi- or single-dose medication vial, or blood glucose monitoring device does NOT mean the item is free from potentially infectious agents.
- All used injection supplies and materials are potentially contaminated and should be discarded.
Proper infection control technique requires that healthcare providers must follow best practice to prevent injury and pathogen transfer. At all times, aseptic technique is to be used to prepare and administer an injection. The following are best practice guidelines.
- Medications should be drawn up in a designated “clean” medication area that is not adjacent to areas where potentially contaminated items are placed.
- Use a new sterile syringe and needle to draw up medications while preventing contact between the injection materials and the non-sterile environment.
- Ensure proper hand hygiene (i.e., hand sanitizing or hand washing if hands are visibly soiled) before handling medications.
- If a medication vial has already been opened, the rubber septum should be disinfected with alcohol prior to piercing it.
- Never leave a needle or other device (e.g., “spikes”) inserted into a medication vial septum or IV bag/bottle for multiple uses. This provides a direct route for microorganisms to enter the vial and contaminate the fluid.
- Medication vials should be discarded upon expiration or any time there are concerns regarding the sterility of the medication.
Never administer medications from the same syringe to more than one patient, even if the needle is changed.
Never use the same syringe or needle to administer IV medications to more than one patient, even if the medication is administered into the IV tubing, regardless of the distance from the IV insertion site.
- All the infusion components from the infusate to the patient’s catheter are a single interconnected unit.
- All the components are directly or indirectly exposed to the patient’s blood and cannot be used for another patient.
- Syringes and needles that intersect through any port in the IV system also become contaminated and cannot be used for another patient or used to re-enter a non-patient specific multidose medication vial.
- Separation from the patient’s IV by distance, gravity and/or positive infusion pressure does not ensure that small amounts of blood are not present in these items.
- Never enter a vial with a syringe or needle that has been used for a patient if the same medication vial might be used for another patient.
Dedicate vials of medication to a single patient, whenever possible.
- Medications packaged as single use must never be used for more than one patient:
- Never combine leftover contents for later use
- Medications packaged as multi-use should be assigned to a single patient whenever possible
- Never use bags or bottles of intravenous solution as a common source of supply for more than one patient
- Never use peripheral capillary blood monitoring devices packaged as single-patient use on more than one patient
- Restrict use of peripheral capillary blood sampling devices to individual patients
- Never reuse lancets. Use single-use lancets that permanently retract upon puncture whenever possible
Safe injection practices and procedures designed to prevent disease transmission from patient to healthcare worker. Fact sheet from OHSA can be found at https://www.osha.gov/OshDoc/data_BloodborneFacts/bbfact01.pdf
Self Quiz
Ask yourself...
- Think back to specific events. What are some high risk practices you've seen take place in your workplace?
Evaluation or Surveillance of Exposure Incidents
A plan to evaluate and follow-up on exposure incidents should be put into place at every facility. At a minimum, this plan should include the following elements:
- Identification of who is at risk for exposure
- Identification of what devices cause exposure
- Education for all healthcare employees that use sharps. This would include that ALL sharp devices can cause injury and disease transmission if not used and disposed properly. Specific focus would include the devices that are more likely to cause injury such as:
- Devices with higher disease transmission risk (hollow bore)
- Devices with higher injury rates (“butterfly”-type IV catheters, devices with recoil action)
- Blood glucose monitoring devices (lancet platforms/pens)
- Identification of areas/settings where exposures occur
- Circumstances in which exposures occur
- Post exposure management - See Element VI
Self Quiz
Ask yourself...
- Is there a plan in place for an exposure response in your workplace?
Engineer Controls
Engineer controls are implemented in order to provide healthcare workers with the safest equipment to complete their jobs. Safer devices should be identified and integrated into safety protocols whenever possible. When selecting engineer controls to be aimed at preventing sharps injuries the following should be considered:
- Evaluate and select safer devices
- Passive vs. active safety features
- Mechanisms that provide continuous protection immediately
- Integrated safety equipment vs. accessory devices:
- Properly educate and train all staff on safer devices
- Consider eliminating traditional or non-safety alternatives whenever possible
- Explore engineering controls available for specific areas/settings
5. Use puncture-resistant containers for the disposal and transport of needles and other sharp objects:
- Refer to published guidelines for the selection, evaluation, and use (e.g., placement) of sharps disposal containers
- National Institute for Occupational Safety and Health (NIOSH) guidelines –
This is available at: http://www.cdc.gov/niosh/topics/bbp/#prevent
- Use splatter shields on medical equipment associated with risk prone procedures (e.g., locking centrifuge lids)
Work Practice Controls
General Practices
- Hand hygiene including the appropriate circumstances in which alcohol– based hand sanitizers and soap and water hand washing should be used (see Element II).
- Proper procedures for cleaning of blood and body fluid spills:
- Initial removal of bulk material followed by disinfection with an appropriate disinfectant.
- Proper handling/disposal of blood and body fluids, including contaminated patient care items.
- Proper selection, donning, doffing, and disposal of personal protective equipment (PPE) as trained [see Element IV].
- Proper protection of work surfaces in direct proximity to patient procedure treatment area with appropriate barriers to prevent instruments from becoming contaminated with blood-borne pathogens.
Preventing Percutaneous Exposures
- Avoid unnecessary use of needles and other sharp objects.
- Use care in the handling and disposing of needles and other sharp objects:
- Avoid recapping unless absolutely medically necessary.
- When recapping, use only a one-hand technique or safety device.
- Pass sharp instruments by use of designated “safe zones.”
- Disassemble sharp equipment by use of forceps or other devices.
- Discard used sharps into a puncture-resistant sharps container immediately after use.
Modify Procedures to Avoid Injury
- Use forceps, suture holders, or other instruments for suturing
- Avoid holding tissue with fingers when suturing or cutting
- Avoid leaving exposed sharps of any kind on patient procedure/treatment work surfaces
- Appropriately use safety devices whenever available:
- Always activate safety features.
- Never circumvent safety features.
Self Quiz
Ask yourself...
- What do you think are the most important procedural factors of Engineer control?
Element IV
Creation and maintenance of a safe environment for patient care in all healthcare settings through application of infection control principles and practices for cleaning, disinfecting, and sterilization.
Element IV Objectives
Upon completion of course work or training on this element, the learner will be able to:
- Describe the circumstances that require the use of barriers and personal protective equipment to prevent patient or healthcare worker contact with potentially infectious material
- Identify specific barriers or personal protective equipment for patient and healthcare worker protection from exposure to potentially infectious material
Definitions
Personal protective equipment (PPE): Specialized clothing or equipment worn by an employee for protection against a hazard.
Barriers: Equipment such as gloves, gowns, aprons, masks, or protective eye wear, which when worn, can reduce the risk of exposure of the health care worker’s skin or mucous membranes to potentially infective materials.
Self Quiz
Ask yourself...
- What tools do you use on a daily basis that require proper sterilization?
Types of PPE or Barriers and Criteria for Selection
Per OSHA guidelines, employers must provide employees with appropriate PPE that provides protection from any potential infectious pathogen exposure (1). PPE includes gloves, cover garb, masks, face shields and eye protection. All PPE is intended to provide a barrier between the healthcare worker and potential contamination, whether from a patient, object, or surface.
Gloves are intended to provide coverage and protection for hands. There are several types of gloves to choose from and the type of patient care or activity should guide choice.
- Sterile – to be utilized when performing sterile procedures and aseptic technique
- Non-sterile – medical grade, non-sterile gloves may be used for general patient care and clean procedures (such as NG tube insertion)
- Utility – not medical grade and should not be used in patient care
Choice in material for gloves is often is dictated by cost and facility preference. When given a choice, considerations should be made as to the types of material being handled.
- Natural rubber latex – rarely used in facilities due to allergen risk
- Vinyl – made from PVC, lower in cost, provides protection in non-hazardous and low-infection environments
- Nitrile – more durable, able to withstand chemical and bio-medical exposure (2)
An appropriately sized glove fits securely over the fingertips and palm without tightness or extra room. If a glove develops a tear or is heavily soiled, it should be replaced immediately.
Cover garb is a protective layer to wear over scrubs or clothes to protect garments and skin. These include laboratory coats, gowns, and aprons. As with gloves, consideration should be given to size, sterility, type of patient care involved, and material characteristics of the gown.
- Fluid impervious – does not allow passage of fluids
- Fluid resistant – resists penetration of fluids, but fluid may seep with pressure
- Permeable – does not offer protection against fluids
Masks are intended to provide protection to the wearers mouth and nose, with respirators providing an extra layer of protection to the respiratory tract against airborne infection pathogens (1).
Goggles are designed to protect the eyes from splashes and droplet exposure, while face shields offer additional protection to the entire face. It is important to note that face shields are not designed to be a replacement for masks.
The choice of PPE is based on the factors that are reasonably anticipated to occur during the patient care encounter. Potential contact with blood or other potentially infectious material can occur via splashes, respiratory droplets, and/or airborne pathogens. The type of PPE chosen will be based on standard or transmission-based precaution recommendations. Follow your facility policy and procedures for guidance on appropriate choice. The nurse will also need to anticipate whether fluid will be encountered, such as emptying a drain or foley collection device. In situations where a large amount of fluid is likely to be encountered, it would be wise to choose a higher level of protection, such as an impermeable gown, if available, and to wear eye protection to ward off splashes.
Choosing Barriers or PPE Based on Intended Need
Barriers and PPE is aimed at keeping patients and healthcare providers safe. There are certain circumstances where specific PPE is selected based on patient care or circumstances.
Patient Safety
Barriers, PPE, and hand hygiene is aimed at keeping patients and healthcare providers safe. There are certain circumstances where specific PPE is selected based on patient care or circumstances. This includes, but is not limited to:
Sterile Barriers for Invasive Procedures
During invasive procedures, such as inserting a central line or during a surgery, staff directly involved performing the procedure or surgery must maintain sterility. Appropriate sterile PPE will be selected based on the type of procedure and the patient will be draped in sterile fashion according to recommended guidelines.
Both the patient and caregiver should wear a mask during central line changes, with the caregiver adhering to aseptic technique (1). Specific policies of the organization should be referred to on the selection and donning and doffing of sterile protective equipment during surgical procedures.
Masks for Prevention of Exposure of Droplet Contamination
Patients in droplet precautions pose a significant risk to healthcare workers and visitors. The patient, as well as anyone inside the patient's room, should wear a mask for the most effective prevention of transmission (1). The patient and patient's family must be educated on the importance of adhering to these guidelines while visitation is appropriate. During transport of a patient under droplet precautions, the patient should wear a mask, placed over the top of any oxygen delivery device, if needed.
Employee Safety
Employees must ensure that they are evaluating the types of exposure that is likely to occur during patient care. Selection of PPE and appropriate barriers should consider the following:
Barriers for Prevention of Contamination
Per the CDC, "use of PPE is recommended based on the anticipated exposure to blood, body fluids, secretions, or excretions" (3). The following are CDC guidelines based on the expected type of exposure or precaution; however, clinical judgement should be used based on the situation (all from 5):
Standard precautions are to be used with any potential exposure to blood, mucous membranes, compromised skin, contaminated equipment or surfaces, and body fluids. Barriers may include gloves, gown, and eye and face protection.
Employees must be judicious in identifying any precautions that are placed on a patient (ie. Contact, droplet, airborne) and following recommended PPE guidelines for protecting themselves and other patients.
PPE should be donned prior to going into a patient room and doffed upon exit. PPE must never be worn in the halls or when going from one patient room to the next. All gloves must be changed in between use and hands washed or sanitized upon removal of gloves.
Additionally, whenever possible, social distancing of 6 feet should occur within the work environment. When not possible, adherence to mask guidelines is sufficient.
Masks for Prevention of Exposure to Communicable Disease
With the onset of Covid-19 across the globe, masks are an essential tool in preventing the transmission of communicable disease. At a minimum, medical masks should be donned during all patient care. During procedures or surgery, surgical masks are to be utilized.
N-95 masks are reserved for patient care with known or suspected Covid-19, if airborne precautions are ordered, or during procedures that may aerosolize (such as during intubations and certain endoscopy procedures). The CDC recommends reserving surgical N-95 masks for healthcare providers "who are working in a sterile field or who may be exposed to high velocity splashes, sprays, or splatters of blood or body fluids". Standard N95 respirators are recommended for all other care involving confirmed or suspected Covid-19 patients (5).
Guidance on Proper Utilization of PPE or Barriers
Proper fit is required for PPE to be effective. Gowns and gloves chosen should fit well, allow movement, and neither be too baggy or too tight. For particulate respirators, the CDC recommends the following regarding proper fit and use of particulate respirators:
All workers who are required to wear tight-fitting respirators (e.g., N95 respirators, Elastomerics) must have a medical evaluation to determine the worker’s ability to wear a respirator, and if medically cleared, a respirator fit test needs to be performed using the same model available in the workplace (3, 4).
Prior to donning PPE, it should be inspected for any anomalies, tears, or vulnerable spots. PPE that is compromised should be disposed of and a new garment selected. Nurses must give careful consideration to the selection of PPE to ensure that it is the correct type for the job and anticipate any circumstances where splashes or saturation of fabric is likely to occur.
The PPE provided by the employer may be single use or re-usable. Always verify with manufacturer guidelines and facility policy on the correct usage and processing of worn garments. It is the facilities responsibility to ensure that re-usable gowns are laundered according to State guidelines.
In order to prevent cross contamination, OSHA offers the following guidelines:
- Personal protective equipment must be removed prior to leaving a work area
- Garment penetrated by blood or other potentially infectious material must be removed immediately or as soon as possible
- PPE must be discarded in “. . . an appropriately designated area or container for storage, washing, decontamination, or disposal”
- Employers must ensure that proper hand washing is taking place after the removal of PPE
Healthcare facilities have a legal duty to protect their workers. Per OSHA, “One way the employer can protect workers against exposure to blood-borne pathogens, such as hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV), the virus that causes AIDS, is by providing and ensuring they use personal protective equipment, or PPE. Wearing appropriate PPE can significantly reduce risk, since it acts as a barrier against exposure. Employers are required to provide, clean, repair, and replace this equipment as needed, and at no cost to workers” (5).
Employers and healthcare workers must understand the balance of cost versus benefit ratio in PPE selection and use. While it is important to be good stewards with resources, always erring on the side of caution and choosing PPE based on anticipated exposure risk is the most effective way to protect yourself and your patients.
For selection, donning, doffing, and disposal refer back to Element II.
Self Quiz
Ask yourself...
- Can you name some appropriate barriers for invasive procedures?
Element V
Creation and maintenance of a safe environment for patient care in all healthcare settings through application of infection control principles and practices for cleaning, disinfecting, and sterilization.
Element V Objectives
At the conclusion of course work or training on this element, the learner will be able to:
- Define cleaning, disinfection, and sterilization
- Differentiate between noncritical, semi critical, and critical medical devices
- Describe the three levels of disinfection (i.e., low, intermediate, and high)
- Recognize the importance of the correct application of reprocessing methods for assuring the safety and integrity of patient care equipment in preventing transmission of blood-borne pathogens
- Recognize the professional’s responsibility for maintaining a safe patient care environment in all healthcare settings
- Recognize strategies for, and importance of, effective and appropriate pre-cleaning, chemical disinfection, and sterilization of instruments and medical devices aimed at preventing transmission of blood-borne pathogens.
Definitions
Contamination: The presence of microorganisms on an item or surface.
Cleaning: The process of removing all foreign material (i.e., dirt, body fluids, lubricants) from objects by using water and detergents or soaps and washing or scrubbing the object
Critical device: An item that enters sterile tissue or the vascular system (e.g., intravenous catheters, needles for injections). These must be sterile prior to contact with tissue.
Decontamination: The use of physical or chemical means to remove, inactivate, or destroy blood-borne pathogens on a surface or item to the point where they are no longer capable of transmitting infectious particles.
Disinfection: The use of a chemical procedure that eliminates virtually all recognized pathogenic microorganisms but not necessarily all microbial forms (e.g., bacterial endospores) on inanimate objects.
High level disinfection: Disinfection that kills all organisms, except high levels of bacterial spores, and is affected with a chemical germicide cleared for marketing as a sterilant by the U.S. Food and Drug Administration (FDA).
Intermediate level disinfection: Disinfection that kills mycobacteria, most viruses, and bacteria with a chemical germicide registered as a “tuberculocide” by the U.S. Environmental Protection Agency (EPA).
Low level disinfection: Disinfection that kills some viruses and bacteria with a chemical germicide registered as a hospital disinfectant by the EPA.
Noncritical device: An item that contacts intact skin but not mucous membranes (e.g., blood pressure cuffs, oximeters). It requires low level disinfection.
Semi critical device: An item that comes in contact with mucous membranes or non-intact skin and minimally requires high level disinfection (e.g., oral thermometers, vaginal specula).
Sterilization: The use of a physical or chemical procedure to destroy all microbial life, including highly resistant bacterial endospores.
Self Quiz
Ask yourself...
- What is the professional’s responsibility for maintaining a safe patient care environment in all healthcare settings?
Universal Principles
Instruments, medical devices, and equipment should be managed and reprocessed according to the recommended and appropriate methods regardless of a patient’s diagnosis, except for cases of suspected prion disease.
Due to the infective nature and steam resistant properties of prion diseases, special procedures are required for handling brain, spinal, or nerve tissue from patients with known or suspected prion disease (e.g., Creutzfeldt-Jakob disease [CJD] or Bovine spongiform encephalopathy [BSE]). Consultation with infection control experts prior to performing procedures on such patients is warranted.
Industry guidelines as well as equipment and chemical manufacturer recommendations should be used to develop and update reprocessing policies and procedures. Written instructions must be made available for each instrument, medical device, and equipment reprocessed. The CDC recommends that critical medical and surgical devices and instruments that would be expected to enter a system through body fluids, blood, or tissue be sterilized prior to use on each patient. (1).
Potential for Contamination
The type of instrument, medical device, equipment, or environmental surface creates variables that are more likely to be a source of contamination. External contamination may be caused by the presence of hinges, crevices, or multiple interconnecting pieces. If able, these devices should be disassembled. Endoscopes provide a particular challenge for both internal and external contamination, due to their lumens as well as the crevices and joints present. The disinfectant must reach all surfaces and assurance that there are no air pockets or bubbles to impede penetration (2). These devices may be made of material that is not heat resistant, preventing sterilization. In these instances, chemicals must be utilized to provide disinfection.
Once rendered sterile, there are multiple opportunities for potential contamination due to the frequency of hand contact with the device or surface. Packaging may be over handled and breached, or the item may come into contact with potential contaminants via poor storage, improper opening, or environmental factors.
The efficacy of sterilization and disinfection is dependent upon the number and type of microorganisms present. There are several types of pathogens that carry an innate resistance, making successful decontamination more challenging (2). Most infections are caused by bacteria, followed by viruses, fungi, protozoa, and prions (3). Due to the nature of their outer membranes, spores and gram-negative bacteria have a natural barrier that prevents the absorption of disinfectants. Bacterial spores are especially resistant against chemical germicides, as are the following pathogenic organism types (all from 2):
- Coccidia – i.e., Cryptosporidium
- Mycobacteria – i.e., M. tuberculosis
- Nonlipid or small viruses – i.e., poliovirus, coxsackievirus
- Fungi – i.e., Aspergillus, Candida
- Vegetative bacteria – i.e., Staphylococcus, Pseudomonas
- Lipid or medium-size viruses – i.e., herpes, HIV
The number of microorganisms that are present on a medical instrument, device or surface affects the time that must be factored into disinfection and sterilization efficacy. As stated by the CDC, “Reducing the number of microorganisms that must be inactivated through meticulous cleaning, increases the margin of safety when the germicide is used according to the labeling and shortens the exposure time required to kill the entire microbial load” (2)
In general, used medical devices are contaminated with a relatively low bioburden of organisms. Inconsistencies or incorrect methods of reprocessing can easily lead to the potential for cross-contamination (1).
Steps of Reprocessing
Reprocessing medical instruments and equipment is completed sequentially dependent upon the instrument and the process chosen.
Pre-cleaning is the process of removing soil, debris, lubricants from internal and external surfaces through mopping, wiping, or soaking. It must be done as soon as possible after use to lower the number of microorganisms present on the object.
Cleaning may be accomplished manually or mechanically. Manual cleaning relies upon friction and fluidics (fluids under pressure) to remove debris and soil from inner and outer surfaces of the instrument. There are several different machines used in mechanical cleaning including ultrasonic cleaners, washer-disinfectors, washer-sterilizers, and washer-decontaminators. Studies have shown that automated cleaning is more effective than manual; however, the frequency of fluid changes must follow manufacturer guidelines to eliminate the risk of contaminating debris (1).
Disinfection involves the use of disinfectants, either alone or in combination, to reduce microbial count to near insignificant. Common disinfectants used in the healthcare setting include chlorine and chlorine compounds, hydrogen peroxide, alcohols, iodophors, and quaternary ammonium compounds, among others. These products are formulated and then approved by the Environmental Protection Agency and Food and Drug Administration for specific uses.
Sterilization is used on most medical and surgical devices that are utilized in healthcare facilities. This requires sufficient exposure time to heat, chemicals, or gases to ensure that all microorganisms are destroyed.
Choice/Level of Reprocessing Sequence
The choice or level of reprocessing is based on intended use:
- Critical instruments and medical devices require sterilization
- Semi critical instruments and medical devices minimally require high level disinfection
- Noncritical instruments and medical devices minimally require cleaning and low-level disinfection.
Manufacturer recommendations must always be consulted to ensure that appropriate methods, actions, and solutions are used. There is a wide variability of compatibility among equipment components, materials, and chemicals used. Rigorous training is required to appropriately to understand equipment heat and pressure tolerance as well as the time and temperature requirements for reprocessing. Failure to follow manufacturer recommendations may lead to equipment damage, elevated microbial counts on instruments after reprocessing, increase risk for infections, and possibly patient death.
Effectiveness of Reprocessing Instruments, Medical Devices, and Equipment
Pre-cleaning and cleaning prior to disinfection is one of the most effective ways to reduce the microbial count. This is only effective when completed prior to disinfection. Disinfection relies upon the action of products to eliminate microbial count. Depending on the medical instrument or device design, the product may only be required to cover the surface. However, due to the lumens of scopes, crevices, or hinges on certain instruments, immersion products and dwell times may be required (4).
The presence of organic matter, such as blood, serum, exudate, lubricant, or fecal material can drastically reduce the efficacy of a disinfectant. This may occur due to the presence of a barrier or the organic material acting as a barrier. It may also occur from a chemical reaction between the organic material and the disinfectant being utilized.
Biofilms pose a particular challenge and offer protection from the action of disinfectants. Biofilms are composed of microbes that build adhesive layers onto the inner and outer surfaces of objects, including instruments and medical devices, rendering certain disinfectants ineffective. Chlorine and Monochloramines remain effective against inactivating biofilm bacteria (1).
Per the CDC, “. . . a given product is designed for a specific purpose and is to be used in a certain manner. Therefore, users should read labels carefully to ensure the correct product is selected for the intended use and applied efficiently” (1). The label will indicate the sufficient contact time with chemical solution to achieve adequate disinfection.
After disinfection, staff and management must adopt a system of record keeping and tracking of instrument usage and reprocessing. Reprocessing equipment must be on a schedule to be maintained and regularly cleaned, according to manufacturer guidelines.
There are several methods of sterilization used such as steam sterilization (autoclaves), flash sterilization, and more recently, low-temperature sterilization techniques created for medical devices that are heat sensitive. Selection depends upon the type of instrument, material, ability to withstand heat or humidity, and targeted microbes.
There are several methods of ensuring that sterilized instruments are processed and tracked appropriately. Indicators or monitors are test systems that provide a way of verifying that the sterilization methods were sufficient to eradicate the regulated number of microbes during the process. These safeguards include:
- Biologic monitors
- Process monitors (tape, indicator strips, etc.)
- Physical monitors (pressure, temperature gauges)
- Record keeping and recall/ tracking system for each sterilization processing batch/item
Studies have shown that the best-practice of handling and storage of reprocessed medical equipment and instruments uses a system of event-related shelf life, rather than time-related. The rationale for this lies in the theory that the sterile items are remaining sterile as long as the packaging is not compromised (2). Factors that are considered event-related include internal or external contamination such as damage to packaging, humidity, insects, vermin, open shelving, temperature fluctuations, flooding, location, and the composition of packaging material
Standards for handling must also focus on protection of workers from health issues.
Recognizing Potential Sources of Cross-Contamination in the Healthcare Environment
- Surfaces or equipment which require cleaning between patient procedures/treatments
- Practices that contribute to hand contamination and the potential for cross-contamination
- Consequences of reuse of single use/disposable instruments, medical devices, or equipment
Factors that Have Contributed to Contamination in Reported Cases of Disease Transmission
At any point in reprocessing or handling, breaks in infection control practices can compromise the integrity of instruments, medical devices, or equipment. Specific factors include:
- Failure to reprocess or dispose of items between patients
- Inadequate cleaning
- Inadequate disinfection or sterilization
- Contamination of disinfectant or rinse solutions
- Improper packaging, storage, and handling
- Inadequate/inaccurate record keeping of reprocessing requirements
Expectations of Health Professionals Based on Setting and Scope of Practice
Professionals who practice in settings where handling, cleaning, and reprocessing equipment, instruments, or medical devices is performed elsewhere (e.g., in a dedicated Sterile Processing Department) are responsible of understanding these core concepts and principles:
- Standard and Universal Precautions (e.g., wearing of personal protective equipment)
- Cleaning, disinfection, and sterilization (Sections III and IV above)
- Appropriate application of safe practices for handling instruments, medical devices, and equipment in professional practice
- Designation and physical separation of patient care areas from cleaning and reprocessing areas is strongly recommended
- Verify with those responsible for reprocessing what steps are necessary prior to submission of pre-cleaning and soaking
Professionals who have primary or supervisory responsibilities for equipment, instruments, or medical device reprocessing (e.g., Sterile Processing Department staff or clinics and physician practices where medical equipment is reprocessed on-site) are responsible for understanding these core concepts and principles:
- Standard and Universal Precaution
- Cleaning, disinfection, and sterilization described in Sections III and IV above
- Appropriate application of safe practices for handling instruments, medical devices, and equipment in professional practice
- Designation and physical separation of patient care areas from cleaning and reprocessing areas is strongly recommended
Facilities must be fastidious in developing appropriate reprocessing practices that follow regulatory guidelines. When selecting appropriate methods, consideration must be given to the antimicrobial efficacy, time constraints and requirement of these methods, as well as compatibility. Compatibility among equipment/materials includes the corrosiveness, penetrability, leaching, disintegration, heat tolerance, and moisture sensitivity.
The toxicity of the products used can pose occupational and environmental hazards to staff and patients. Facilities must adopt policies and procedures to reduce exposure to harmful substances, monitor for harmful exposures, and train staff on reprocessing cleaning and chemicals. To reduce potential exposure to harmful substances, OSHA mandates that training for workers prior to use include (all from 5):
- Health and physical hazards of the cleaning chemicals
- Proper handling, use, and storage of all cleaning chemicals being used, including dilution procedures when a cleaning product must be diluted before use
- Proper procedures to follow when a spill occurs
- Personal protective equipment required for using the cleaning product, such as gloves, safety goggles and respirators
- How to obtain and use hazard information, including an explanation of labels and SDSs
Other considerations in developing a safety plan for appropriate reprocessing practices include:
- Potential for patient toxicity/allergy
- Residual effects including antibacterial residual and patient toxicity/allergy
- Ease of use
- Stability of products, including concentration, potency, efficacy of use, and effects of organic material
- Odor
- Cost
- Monitoring requirements and regulations
- Specific labeling requirements for reprocessing single-use devices (specific information may be obtained at https://www.fda.gov/media/71405/download)
Self Quiz
Ask yourself...
- List some bacterial spores that are chemically resistant.
Element VI
Prevention and control of infections and communicable diseases in healthcare workers.
Element VI Objectives
At the conclusion of course work or training on this element, the learner will be able to:
- Recognize the role of occupational health strategies in protecting healthcare workers and patients
- Recognize non-specific disease findings that should prompt evaluation of healthcare workers
- Identify occupational health strategies for preventing transmission of blood-borne pathogens and other communicable diseases in healthcare workers
- Identify resources for evaluation of healthcare workers infected with HIV, HBV, and/or HCV
Definitions
Infectious Disease: A clinically manifest disease of humans or animals resulting from an infection.
Communicable Disease: An illness due to a specific infectious agent or its toxic products that arises through transmission of that agent from an infected person, animal, or inanimate source to a susceptible host.
Occupational Health Strategies: As applied to infection control, a set of activities intended to assess, prevent, and control infections and communicable diseases in healthcare workers.
Pre-Placement and Periodic Health Assessments
Occupational health strategies are aimed at ensuring that employees are healthy and stay healthy. Upon hiring, employees should undergo an initial health screening that reviews immunization records. The CDC suggests that healthcare workers are screened when newly hired and on a periodic basis to (all from 1):
- Ensure sufficient immunity to vaccine-preventable diseases such as measles, mumps, rubella, varicella, hepatitis B, annual influenza and any other recommended or mandated requirements
- Assess for and manage underlying conditions and illness that may affect workplace safety
- Prevent, assess, and treat any potential infectious exposures or illness that may be acquired or transmitted within the healthcare setting
- Initiate and continue personalized health counseling
- Thorough history and physical
A tuberculosis screening should be completed prior to new employees providing patient care and upon possible exposure for an existing employee. A thorough assessment should include an evaluation of the following symptoms:
- Fever
- Cough
- Chest pain, or pain with breathing or coughing
- Night sweats
- Chills
A Mantoux tuberculin skin testing (TST) must also be completed. The test is performed by injecting a small amount of tuberculin to the epidermis of the forearm. The test is then evaluated for a reaction in 48 to 72 hours. If there is no reaction, the test result is negative. If reactive, a scale is used to interpret the measurement of induration and to direct further testing or treatment (2).
When working in healthcare, nursing staff must be healthy to provide optimal care. This is especially true with vulnerable patients that have weakened immune symptoms. The following symptoms require immediate evaluation by a licensed medical professional:
- Fever
- Cough
- Rash
- Vesicular lesions
- Draining wounds
- Vomiting
- Diarrhea
Upon evaluation, there may be restriction from patient care activities and work clearance must be completed prior to a return.
Management Strategies for Potentially Communicable Conditions
Management and the Infection Prevention department should collaborate and strategize to ensure that employees that have had an exposure or possible exposure are protected and have support in seeking treatment without fear of retaliation or job loss (3). Managerial support should prioritize:
- Appropriate evaluation and treatment
- Limiting contact with susceptible patients and staff
- Placement in a non-clinical setting
- Depending on severity of symptoms or potential transmission, a furlough until noninfectious may be necessary
Specific Occupational Health Strategies for Prevention and Control of Blood-borne Pathogen Transmission
Robust training and educational programs are essential for the prevention of healthcare worker exposure and transmission. Prevention strategies should include education, training, and availability of the following:
- Information on potential agents such as HBV, HCV, and HIV
- HBV vaccination (including safety, efficacy, components, and recommendations for use)
- Hand hygiene
- Appropriate PPE and barrier precautions (see Element II)
- Sharps safety (see Element III)
- Standard and Universal Precautions
- Education on the availability of confidential and anonymous testing for blood borne pathogens (4)
Post-Exposure Evaluation and Management
Each facility must make a plan for post-exposure evaluation and management in the case that any employee or patient experiences a potential or actual blood borne exposure. The plan should incorporate the following:
- Prompt evaluation by licensed medical professional
- Risk assessment in occupational exposures
- Recommendations for approaching source patient and healthcare worker evaluations
- Recommendations for post-exposure prophylaxis emphasizing the most current CDC guidelines
- Post-exposure management of patients or other healthcare workers when the exposure source is a healthcare worker requires that the patient be informed of the type of exposure, whether it is healthcare worker’s blood or other potentially infectious material.
Airborne or droplet pathogens require several special considerations. The below guidelines should be applied appropriately.
- Risk of exposure or illness
- Testing
- Options for and risks and benefits of post-exposure prophylaxis or treatment
- Need for specialty care
- Follow-up testing and treatment
- Work restrictions, if indicated
- Risk of transmitting infections to others and methods to prevent transmission, and
- Signs and symptoms of illness to report after an exposure, including side effect of prophylaxis.
Evaluation of Healthcare Workers Infected with HIV, HBV, HCV and/or other Blood-borne Pathogens
The CDC provides the following recommendations based on scientific evidence-based practice in relation policies to prevent infected health care personnel-related blood-borne pathogen transmission (3).
- Strict adherence to Standard Precautions
- Voluntary testing without fear of disclosure or discrimination
- There is not mandatory screening of healthcare workers for blood-borne pathogens in every state. Such a program would cost millions of dollars and would not produce any appreciable gain in public safety. Negative antibody tests for HIV, HBV, and HCV do not rule out the presence of infection since it can take some time for measurable antibodies to appear.
Criteria must be followed when evaluating infected health care workers for risk of transmission in order to adhere to laws protecting workers from discrimination. The following outlines a general assessment to determine the risks posed:
- Nature and scope of professional practice
- Techniques used in performance of procedures that may pose a transmission risk to patients
- Assessed compliance with infection control standards
- Presence of weeping dermatitis, draining or open skin wounds
- Overall health:
- Physical health – ability to carry out duties with Cognitive status
Self Quiz
Ask yourself...
- As a healthcare worker, did you see a growing need for healthcare workers to be evaluated during the pandemic?
Element VII
Sepsis Awareness and Education
Element VII Objectives
At the conclusion of course work or training on this element, the learner will be able to:
- Describe the scope of the sepsis problem
- Describe persons at increased risk of developing sepsis
- Identify common sources of infection that may lead to sepsis
- Describe early signs and symptoms that may be associated with sepsis in adults and children and infants
- Understand the need for immediate medical evaluation and management if sepsis is suspected
- Educate patients and families on methods for preventing infections and illnesses that can lead to sepsis and on identifying the signs and symptoms of severe infections and when to seek medical care
Definitions
Sepsis: a life-threatening condition caused by a host’s extreme response to infection. The Surviving Sepsis Campaign 2016 International Guidelines define sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection. Earlier definitions defined sepsis as an inflammatory response to infection, while sepsis associated with organ dysfunction was identified as severe sepsis.
Septic shock: a subset of sepsis that manifests with circulatory and cellular/metabolic dysfunction; it is associated with a higher mortality risk.
Sepsis – Scope of the Problem
Over 1.7 million Americans are diagnosed with sepsis each year, with the incidence rising by approximately 8% annually. Sepsis is a life-threatening medical emergency that requires early recognition and intervention. Sepsis occurs when the body overcompensates in response to an infection, resulting in multiple organ dysfunction and damage. Most sepsis cases are community-acquired. Early recognition and treatment are the most effective ways to combat sepsis.
In 2013, New York State became the first in the U.S. to develop a state mandate that requires all hospitals to develop and adopt sepsis protocols. The mandate is dubbed “Rory’s Regulations,” after Rory Staunton, a 12-year-old boy whose death was attributed to lack of sepsis recognition. These protocols were required to adopt the following practices (all from 2):
- A process for the screening and early recognition of patients with sepsis, severe sepsis, and septic shock
- A process to identify and document individuals appropriate for treatment through severe sepsis protocols, including explicit criteria defining those patients who should be excluded from the protocols, such as patients with certain clinical conditions or who have elected palliative care
- Guidelines for hemodynamic support with explicit physiologic and biomarker treatment goals, methodology for invasive or non-invasive hemodynamic monitoring, and time frame goals
- For infants and children, guidelines for fluid resuscitation with explicit time frames for vascular access and fluid delivery consistent with current evidence-based guidelines for severe sepsis and septic shock with defined therapeutic goals for children
- A procedure for identification of infection source and delivery of early antibiotics with time frame goals
- Criteria for use, where appropriate, of an invasive protocol and for use of vasoactive agents
Medical staff also gained responsibility for the collection, use, and reporting of quality measures and mortality data to peers, including national, hospital and expert stakeholders (2).
Causes of Sepsis
As stated by the Sepsis Alliance, “Sepsis is the body’s overwhelming and life-threatening response to infection that can lead to tissue damage, organ failure, and death” (4). Bacterial infections commonly trigger sepsis, although other microbial infections (e.g., fungal, or viral) can also trigger sepsis. The triggering infection most commonly originates from the lungs, urinary tract, skin, and/or gastrointestinal tract.
Certain populations are at an increased risk of developing sepsis including:
- The very young (under 1 year), and individuals 65 years of age and older
- People with chronic conditions such as diabetes, lung disease, kidney disease, or cancer and
- People with impaired immune systems
Early Recognition of Sepsis
- Manifestations of sepsis vary based on the type of infection and host factors
- Some people may have subtle sepsis presentations
- Signs and symptoms that may be associated with sepsis in persons with confirmed or suspected infection can include:
- Altered mental state
- Shortness of breath
- Fever
- Clammy or sweaty skin
- Extreme pain or discomfort
- High heart rate
Signs and symptoms in children and the elderly may not present the same. In children and the elderly sepsis symptoms may present as above or any of the following: decreased temperature, pallor or bluish tone to skin, non-blanching rash, high respiratory rate, lethargy, and seizure.
Sepsis can progress to more severe forms of sepsis, including septic shock. When septic shock occurs, the body’s inflammatory response causes extensive vasodilation throughout the body. This results in a sudden drop in blood pressure that can quickly lead to organ failure and damage (5).
If a person presents with suspected or confirmed infection, healthcare professionals should assess for signs of, and risk factors for sepsis following facility sepsis protocols.
Principles of Sepsis Treatment
Sepsis treatment starts with a prompt recognition and diagnosis. The diagnosis of sepsis starts with the assessment of a patient with a known or suspected infection. For adults, sepsis is defined as having two or more symptoms of systemic inflammatory response syndrome, which includes (all from 6):
- Temperature (>38 o C or <36 o C)
- Elevated heart rate > 90 bpm
- WBC (<4×109/L or >12×109/L)
- Respiratory rate (>20 breaths/min, PACO2<32 mm Hg
Severe sepsis has traditionally been defined as having sepsis plus organ failure, while septic shock involved sepsis along with refractory hypotension after fluid resuscitation or requiring vasopressors to maintain hemodynamics (6). The standard changed in 2016 with the elimination of severe sepsis; however, most facilities still adhere to the above criteria. Follow sepsis protocol and bundles per facility.
With recognition of sepsis and/or septic shock, previously state law mandated that one- and three-hour care bundles be created. While these may vary slightly per facility, Surviving Sepsis promotes a one-hour bundle that incorporates all the recommendations of the other bundles; yet, decreases the time to treat (all from 7):
One Hour Bundle
- Obtain lactate level. Reorder if initial lactate is > 2 mmol/L
- Obtain blood cultures prior to administering antibiotics
- Administer broad-spectrum antibiotics
- Rapidly infuse crystalloids at a rate of 30 mL/kg for hypotension or lactate ≥ 4 mmol/L
- If hypotensive post fluid resuscitation, administer vasopressors to maintain a mean arterial pressure ≥ 65 mmHg
In addition to blood cultures, type and screens may be ordered for urine, wound exudate, or respiratory secretions depending upon where the suspected infection is originating from. Blood tests may also include a complete blood count and basic metabolic panel to assess for any damage to the kidneys or liver. Other diagnostic imaging may include chest x-ray, CT, ultrasound, and MRI (8).
Fluid resuscitation and vasopressors, if needed, will continue until the patient is hemodynamically stable. Physicians should be notified when blood cultures result in order to ensure that the ordered antibiotic is effective against the identified organism (8).
Patient Education and Prevention
Patient education should strive to provide memorable and simple ways to stay free of infection. The number one method of preventing infection is adequate hand hygiene. The CDC also suggests that patients keep wounds and cuts clean and covered until healed.
Patients at higher risk should be notified of their risk factors, including (all from 9):
- Adults 65 or older
- People with chronic medical conditions, such as diabetes, lung disease, cancer, and kidney disease
- People with weakened immune systems
- Sepsis survivors
- Children younger than one
Patients should be educated on warning signs and symptoms of sepsis that are easy to remember. The Sepsis Alliance suggests the following acronym and verbiage for seeking immediate care (all from 4):
T - Temperature
I - Infection
M - Mental Decline
E - Extremely Ill
Patients should be encouraged to give relevant history and information to clinicians, including if they have had a recent infection, sepsis in the past, or are immunocompromised.
Self Quiz
Ask yourself...
- What are the lead causes of sepsis?
- How can sepsis be treated?
- How can sepsis be prevented?
PTSD in Nurses
Introduction
Post-Traumatic Stress Disorder (PTSD) gained recognition from its association with Military Veterans in the Vietnam War emotional strain from the events they witnessed after returning home from war. Names like “shell shocked” or “combat fatigue” were used to describe the Veterans upon their return. In 1980, the Diagnostic and Statistical Manual of Mental Health Disorders, developed by the American Psychiatric Association, officially identified this condition as a psychological disorder (4).
Although anyone can experience PTSD, healthcare professionals have an increased risk of presenting with this disorder. Year 2020 has most likely been the most s most stressful year for many people. Many have lost their income, family, homes, and sense of well-being. Emergency personnel, rescue workers, physicians, and nurses have all voiced how COVID-19 has had a terrible impact on everyone. The increase in hospitalization and deaths has caused a major increase in Post-Traumatic Stress Disorder Diagnosis (PTSD) among the general population and healthcare professionals. In this course, we will discuss strategies that healthcare professionals can utilize to promote successful identification and coping mechanisms for PTSD.
Healthcare professionals practice in an environment that is extremely high stressed, demanding, and unpredictable. Nurses, physicians, and other healthcare professionals are continuously exposed to physical, psychological, and mental hazards for upward of 12-16 hours a day. Each person reacts and responds to extreme stress and trauma in various ways. Since there are so many variables to consider, it has been difficult to diagnose PTSD in healthcare professionals.
It is natural for individuals to experience fear, heightened senses, and avoidance after experiencing a traumatic event. Healthcare professionals are aware of the “fight or flight” response – our body’s natural defense to our sense of danger or fear. Everyone has an individual definition of trauma. For some people losing a loved one is considered a traumatic event. For others, the definition of a traumatic event may be coming in contact with an immediate threat on their personal life or witnessing a dangerous situation. When does it turn into PTSD? To understand that question we must first define PTSD.
Case Study
Laura is a 26-year-old new nurse of five years that has decided to take a job doing traveling nursing to help with the overwhelming demand of taking care of COVID-19 patients. She is offered a wonderful opportunity to make a difference. The travel agency offers her a staff nurse position taking care of two patients in the critical care unit. She will work 13 weeks at 36 hours weekly on nights. Her pay is 5,000 per week plus a non-tax stipend for her lodging and meals. She accepts the position and takes leave from her full-time position. She leaves behind her pet dog as she prepares to go to California from Tennessee to begin working at the hospital. The agency contacts her to tell her they will also provide transportation to and from her residence to the hospital at no charge.
Laura arrives in California and reports to the hospital department where she will work. After speaking with the nurse manager, Laura is told that her assignments have changed, and she will still work in the critical care unit but will care for at least seven patients who have COVID-19 because they are so short-staffed. Laura is confused and does not really know if she can say no to the assignments because of her contract. She tries to contact her agency, but no one can take her call. She leaves a message in hopes that someone will return her call. Laura is expected to start work that same evening. She is a little hesitant but reports to duty as scheduled.
Laura's first night is horrific. She must care for seven patients who have COVID-19. The patients are all on ventilators and no one is available as a resource for her to ask questions. The entire environment is overwhelming. Patients are lined against the wall, people are crying, a code red is called every 10 to 15 minutes, and most of the time the patient dies. The morgue is overflowing and some of the deceased patients are placed in body bags and lined against the wall. After three shifts Laura decides she cannot fulfill this contract because she has no support. Lately, she is experiencing nightmares, feels very agitated and anxious, and cries all the time.
Laura reaches out to her agency and informs them of her decision, but she is informed that if she breaks the contract, she will be reported to the board of nursing for job abandonment. Laura decides to stay to fulfill the contract. Laura also notices some of her co-workers are manifesting a change in behavior. They have become increasingly sad, detached from others, and anxious. They are also displaying anger toward other staff members. Laura feels the environment is toxic and wishes she were anywhere but there.
Refer to this case study to answer some questions throughout the course.

Definition
Post-traumatic stress disorder is defined as a psychiatric disorder that can occur in people who have experienced or witnessed a traumatic event (1).
The DSM-5 diagnostic criteria for PTSD include:
A. Stressor (one required):
- Personally experiencing trauma or watching someone endure it.
- Learning that a traumatic event(s) may have occurred to a close family member or friend.
- In cases of life-threatening instances, or the death of a family member/friend, the event(s) must have been violent or accidental.
- Experiencing repeated excessive exposure to adverse effects of a traumatic event (e.g. nurses working in critical care units, caring for COVID-19 patients, etc.) (2).
B. Intrusion symptom (one or more required):
- Recurrent and distressing memories or dreams of the trauma experienced.
- A dissociative reaction in which the person is completely unaware of their surroundings.
- Intense, prolonged psychological exposure to internal or external cues that may resemble the traumatic event.
- Distinct physiological reactions of internal or external reminders that may represent any aspect of the traumatic event (2).
C. Avoidance (one or both required): Avoiding any memories, thoughts, or feelings related to the traumatic event on a continuous basis.
- Avoidance or efforts to avoid instances or items that resemble or remind the person of the traumatic event. Examples include (2):
- People
- Places
- Activities
- Conversations
- Familial objects
D. Negative alteration in cognition and mood (two required):
- Inability to remember specifics of the traumatic event due to dissociative symptoms.
- Persistent and over-exaggerated negative belief about oneself, others, or the world (e.g. “the world is completely dangerous” or “my whole nervous system is shot”).
- Persistent negative emotional state (e.g. fear, anger, guilt, or shame).
- Persistent distorted perception about the cause of the traumatic event leads an individual to blame themselves.
- Distinctive or diminished interest or participation in any significant activities. Feelings of detachment from others. Continuous inability to experience positive emotions (2).
E. Alterations in arousal and reactivity (two or more):
- Angry outbursts and irritable behavior without provocation, leading to physical aggression toward people or objects.
- Self-destructive reckless behavior.
- Hypervigilance.
- Exaggerated startle response.
- Problems with concentrating.
- Sleep disturbance (2).
F. Duration of the disturbance (criteria B, C, D, and E required):
- More than a month.
G. Functional Significance (required):
- Clinically significant distress caused by the traumatic event(s) or impairment in social, occupational, or other areas of functioning.
- The functional disturbance is not attributable to the psychological effects of a substance or any other medical condition (2).
Case Study
Post-Traumatic Stress Disorder (PTSD) is defined as a psychiatric disorder that can occur in people who have experienced or witnessed a traumatic event such as a natural disaster, a serious accident, a terrorist act, war/combat, or rape (1). PTSD also can occur in people who have been threatened with death, experienced sexual violence, sustained a serious injury, continuously works in a highly stressful environment (such as a hospital), or feel helpless in assisting those that have been placed in their care (1).
The DSM-5 diagnostic criteria for PTSD includes the following.
Stressor: (one required)
- Experiencing trauma
- Watching some type of trauma as it occurs to others
- Learning that the traumatic event(s) may have occurred to a close family member or close friend.
- Actual or threatened death of a family member or friend (the event or events must have been violent or accidental).
- Experiencing repeated excessive exposure to adverse effects of a traumatic event (e.g. healthcare professionals working in critical care units, nurses, physicians, paramedics caring for COVID-19 patients) (2).
Intrusion Symptom: (one or more required)
- Recurrent and distressing memories of the trauma experienced
- Recurrent and distressing dreams related to the traumatic event.
- Dissociative reaction in which the person is completely unaware of their surroundings.
- Intense prolonged psychological exposure to internal or external cues that may resemble the traumatic event.
- Distinct physiological reactions of internal or external reminder that may represent any aspect of the traumatic event (2).
Avoidance: (one or both required)
- Avoiding any memories, thoughts, or feelings related to the traumatic event.
- Avoidance or efforts to avoid people, places, activities, conversation, or familial objects that may be a reminder of the traumatic event (2).
Negative Alteration in Cognition and Mood (two required)
- Inability to remember any aspect of the traumatic event due to dissociative symptoms.
- Persistent overexaggerated negative belief about oneself, others or the world (e.g. such as the world is completely dangerous or my whole nervous system is shot).
- Persistent negative emotional state (e.g. fear, anger, guilt or shame).
- Persistent distorted perception about the cause of the traumatic event that leads an individual to blame themselves.
- Distinctive or diminished interest or participation in any significant activities.
- Feelings of detachment from others.
- Continuous inability to experience positive emotions (2).
Alterations in Arousal and Reactivity (two or more)
- Angry outbursts and irritable behavior without provocation, leading to physical aggression towards people or objects.
- Self-destructive reckless behavior.
- Hyper vigilance.
- Exaggerated startle response.
- Problems with concentrating.
- Sleep disturbance (2).
Duration of the Disturbance (Criteria B, C, D, and E required)
More than a month
Functional Significance (required)
- Clinically significant distress caused by the traumatic events or impairment in social, occupational, or other areas of functioning. The functional disturbance is not attributable to the psychological effects of a substance or any other medical condition (2)
Self Quiz
Ask yourself...
- Have you experienced perceived trauma that can be categorized as PTSD?
- Can a person experience PTSD without having a clinical diagnosis?
- Think of Laura’s current work environment. When you are having a stressful day, what do you think she is feeling or thinking?
- How are her co-workers relating to her actions?
Sign and Symptoms
There are many signs and symptoms of PTSD. Symptoms may develop immediately or within three months of the traumatic event(s). On some occasions, a person can suppress their feelings for up to a year before remembering a traumatic event. These signs and symptoms are grouped into four categories: intrusive memories, avoidance, negative changes in mood and thinking, and negative changes in physical and emotional reactions (3).
Intrusive Memories
Intrusive memories include recurrent distressing memories of the traumatic event, flashbacks, nightmares, severe emotional distress, or a physical reaction to something that reminds you of the traumatic event (3)
Avoidance
Avoidance includes cognitively trying to avoid thinking about the traumatic event and avoiding places, activities, conversations, tangible items, and people that reminds you of the traumatic event (3)
Negative Changes in Mood and Thinking
Negative changes in mood and thinking include feelings of hopelessness about the future, memory problems including not remembering certain aspects of the traumatic event, difficulty in maintaining close relationships, feeling of detachment, lack of interest in activities once enjoyed, difficulty experiencing positive emotions, feeling emotionally numb, alcohol abuse, drug abuse, having negative thoughts about yourself or other people around you or the world in general (3).
Changes in Physical and Emotional Reactions
Changes in physical and emotional reactions include being easily startled or frightened, always being on guard for danger, insomnia, trouble concentrating, overwhelming feelings of guilt or shame, increased irritability, aggressive behavior, angry outburst with no provocation, chronic illnesses, gastrointestinal problems, angina, self-destructive behavior, sweating/shaking, heightened “fight or flight” syndrome, pain, depression, hallucinations, anxiety, and feelings of constant sorrow (3).
Self Quiz
Ask yourself...
- Take a mental moment. Do you feel like you are experiencing any of these symptoms or have experienced them in the past?
- As a nurse, can you identify any of these symptoms in your co-workers? Does Laura or her co-workers display any of these symptoms?
- How many times have you brushed off any of these symptoms as just isolated events?
Types of PTSD
Since we know that the American Psychiatric Association describes PTSD as an anxiety disorder, we know there are different types and severity of PTSD. The types of PTSD are categorized according to the severity of the symptoms to help with the diagnosis. There are five types of PTSD which include: Normal stress response, Acute Stress disorder, Uncomplicated PTSD, Complex PTSD, and Comorbid PTSD (5).
Normal Stress Response
The normal stress response, the “fight or flight” syndrome is the precursor to PTSD, and it does not always lead to full blown PTSD. Any event that causes the natural stress response (such as surgery, an injury, or pending thoughts of danger), initiates a normal stress response. The problem occurs when this response is not alleviated within a short amount of time.
Acute Stress Disorder
A life-threatening event such as job loss, illness, natural disaster, or death of loved one can initiate this early form of PTSD. While the individual may experience this type of disorder, the individual will usually overcome the initial stressor. If it becomes prolonged and untreated, it can lead to full blown PTSD.
Uncomplicated PTSD
This type of PTSD is associated with one major event which makes it the easiest form of PTSD to treat. The individual will want to avoid anything that may remind them of the event.
Complex PTSD
Complex PTSD is just as the name implies. This type of PTSD is associated with multiple traumatic events and is usually associated with various types of abuse, violence, war, and traumatic losses. The unfortunate problem with diagnosing this type of PTSD is that some health care professionals confuse it with borderline or antisocial personality disorder or dissociative disorders (5).
Comorbid PTSD
This type of PTSD is associated with a person that has more than one mental health concern along with substance or narcotic misuse issues at the same time. This condition is extremely common because most people have more than one problem. What makes this type of PTSD more complicated to treat is the fact that individuals try to self-medicate because they are in denial, but this only leads to self-loathing and self-destructive behaviors (5).

Self Quiz
Ask yourself...
-
Can you identify with any one of the types of PTSD listed?
-
If any, which type of PTSD might Laura be experiencing? What about her co-workers?
-
How difficult would it be to recognize the difference between the five types of PTSD within yourself or your co-worker?
Phases of PTSD in Nurses
There are four phases of PTSD identified by Pyramid Health. The phases are the impact phase (emergency), rescue phase, the intermediate recovery phase and the long-term reconstruction phase (6).
Impact Phase (Emergency)
The impact phase consists of the initial reaction such as anxiety, helplessness, guilt, shock, or fear. This is the first phase which occurs immediately after the individual experiences the traumatic event. The length of time the individuals stays in this phase depends on the severity of the traumatic event (6).
Rescue Phase
The rescue phase involves the affected person being able to come to terms with what has happened. This phase is closely related to the acceptance phase in grieving. The individual may experience flashbacks, confusion, anxiety, denial, or feelings of despair.
Intermediate Recovery Phase
The intermediate recovery phase is associated with the individual making the adjustment to return to normal everyday life. In this phase, the individual can begin to look at other issues within their life. While they are addressing new issues, they may have the feeling of altruism in which they feel the love and support from others which gives them the sense that they can also help others. They may also develop the feeling of disillusionment in which they feel overwhelmed because they are not receiving the love and support they think they should, or when the love and support ends, they realize they are on their own. This phase is also closely related to the acceptance phase in grieving. As with the grieving phase the individual may go back and forth between phases.
Long-term Reconstruction Phase
The long-term reconstruction phase is characterized by the individual being able to rebuild while dealing with the trauma's aftermath. Their main concern is about their future and how they can maintain healing.
Causes of PTSD
Defining the causes of PTSD can be quite difficult because physicians have not been able to determine why some individuals may have a different response to the same traumatic event. Most adults have experienced some stressful experiences that did not cause PTSD. Some causes of and risk factors for PTSD could include inherited mental health risk, an individual's temperament, and even the way our brain regulates chemicals and hormones which release stress in our bodies.
Considerable evidence links the hippocampus to the representation of contexts by the brain suggesting that the hippocampus has a central role in solving the equivalence problems with respect to content. Tracking moment-to-moment change in input and detecting change sufficient to require altering behavior is crucial to survival. This perspective highlights the critical role of the hippocampus in both spatial cognition, episodic memory tracking change, and detecting boundaries separating context or episode from another. This is very important in people that suffer with PTSD (14).
The hippocampus is a component of the brain, a part of the lymphatic system that plays a role in the consolidation of information from short-term memory to long-term memory, linking memories to sensations and in spatial memory that enables navigation (9, 14). The hippocampus is located under the cerebral cortex in the allocortex and there are two hippocampi, one on each side of the brain. Post-traumatic stress disorder is associated with abnormal hippocampal activity (9, 14). It has been noted that PTSD is mainly associated with functional and structural changes in the amygdala, medial prefrontal cortex, and the hippocampus (9, 14).
The two hippocampi have very distinct roles. The posterior hippocampus' main role is in memory retrieval and spatial cognition. The anterior hippocampus role is mainly associated with the amygdala, the hypothalamic-pituitary-adrenal (HPA) axis, and the limbic prefrontal circuitry (9, 14). The anterior hippocampal-amygdala connections are thought to underlie atypical memory processes in PTSD, including flashbacks, intrusive thoughts, and nightmares (9, 14). There are current theories of PTSD that identify hippocampal dysfunction as a key contributor to hallmark symptoms of PTSD (9, 14).
One common denominator for causes of PTSD is the actual stress an individual goes through when they experience or learn about a life-threatening event, serious injury, sexual assault, childhood physical abuse, being threatened with a weapon, an accident, being exposed repetitively to death, violence, or sickness.
The outbreak of COVID-19 has caused a rise in PTSD in healthcare professionals. Working tirelessly to care for patients experiencing new health issues caused by COVID-19 has put so much pressure on healthcare professionals trying to save their lives.
Unfortunately, because there is no cure for COVID-19 and the public does not always follow the guidelines to prevent the spread of COVID-19, paramedics, doctors, nurses, and other healthcare professionals are continuously putting their own and their families’ lives at risk to try and save lives. This amount of pressure has increasingly led to a spike in PTSD among healthcare workers.
Healthcare workers in critical care, trauma, and the emergency room continuously witness death while operating in a crowded setting and working with an uninterrupted circadian rhythm due to being short staffed. The healthcare workers’ age, years of work experience, family support, marital status, and coping styles along with prior psychiatric history all play a role in the time they may experience PTSD and what type they will experience. The feelings of helplessness that the healthcare worker experiences when trying to care for the patient who has COVID-19 is a major precursor to the development of full-blown PTSD because they may feel conflicted. They want to help their patients get better, but instead they witness them die alone upwards to every five minutes depending on the department in which they are working.
Prevalence of PTSD Among Healthcare Workers
Based on the current U.S. population, around 7 or 10 of every 100 (7% - 8% people) will have experienced some traumatic event in their lifetime and this equates to approximately 223.4 million people. Of that amount, currently 20% (44.7 million people) suffer from PTSD. About every 10 out of every 100 (10%) women develop PTSD sometimes in their life compared to about four of every 100 (4%) men. This makes women twice as likely to develop PTSD (11).
Nurses at the forefront during the pandemic are likely to have experienced major trauma. Such traumas included increased (nearly impossible) workloads, poor patient outcomes, and virtually no support system availability. These traumas led to depression. anxiety and increased cases of PTSD (10).
Healthcare professionals are trained to take care of the needs of their patients and leave their personal feelings at the door. When the shift starts, the healthcare professional suppresses their emotions so they can get through their shift. The problem arises when the shift is over and the healthcare professional may experience a rush of feelings such as anger, guilt, confusion, sadness, sorrow, and grief. Sometimes in extreme cases, they may experience suicidal or homicidal ideations. To mask their emotions, they may turn to drinking, drugs, or destructive behaviors to cope with the day-to-day trauma.
A 2021 study in Occupational Health and Safety revealed that during the outbreaks of severe acute respiratory syndrome (SARS), Middle East respiratory syndrome coronavirus (MERS-CoV) and COVID- 19, the development of PTSD ranged between 11% and 73.4% with 51.5% of healthcare professionals and nurses scoring above the Event Scale -Revised (IES-R) threshold for PTSD diagnosis. It was also found that healthcare professionals and nurses during the COVID-19 pandemic have had a higher rate of PTSD symptoms (71.5% - 73%) when compared to rates during the SARS outbreak, which were at only 5% (10).
One study predicted that approximately 10% - 40% of nurses will have a manifestation of PTSD between one and three years after a pandemic. Poor working conditions and the possibility of COVID-19 exposure had a clear negative impact on nurses' mental health, thus increasing the rate of PTSD (12).
Young female workers, much of the nursing workforce, who lacked social support due to social distancing restrictions were at a higher risk of developing PTSD. In addition to the social distancing protocols, nurses may have experienced further stress due to self-imposed isolation practices to keep their families from exposure to COVID. This contributed to an even greater percentage of nurses being affected by PTSD (13).
The nurses that experienced PTSD were in leadership roles, possessed a negative perception of patient care, lacked supportive relationships to work and at home, experienced longterm patient suffering and internalized patient suffering, experienced lack of staffing frequently and lack of organizational support (15). Post-traumatic stress disorder is highly prevalent among healthcare professionals during and after a pandemic, disaster, or tragic event.

Self Quiz
Ask yourself...
- Would Laura’s symptoms or actions lead you to think she was experiencing PTSD?
- What about her co-workers, would their actions lead you to think they were experiencing PTSD?
- Do the statistics in the section above make a difference in your assessment of Laura’s symptoms?
Global Impact
The current outbreak of the COVID-19 infection and the surgency of new mutant strains from the original strand has spread around the world and caused great concern for global and mental health. This current virus, like others before it, has caused an increase in anxiety, stress, economic decline, anger, and most of all fear. This virus has likely touched everyone in the world in some form or fashion due to the isolation that had become the norm.
While reportedly 92,026,654 people have recovered from the virus, there are long-lasting effects they now must live with whether physical or mental (16). The sheer numbers can cause panic in healthcare professionals.
In 2003, the SARS-CoV outbreak in Singapore caused a rise of PTSD by 27%. After the 2015 MERS Korean outbreak, the Ebola outbreak in Sierra Leone in 2014 and the Ebola outbreak in 2015 in the Democratic Republic of the Congo, the cases of PTSD in healthcare workers increased significantly because they were on the front lines and had heighten symptoms (17).
A multinational study that included 906 healthcare workers across the globe taking care of patients who had COVID-19 concluded that the healthcare workers that participated screened positive for moderate to severe depression (5.3%) and moderate to extremely severe stress (3.8%). The prevalence of physical and psychological symptoms such as stress, depression, anxiety leading to PTSD were increased in the healthcare workers (18).
A study conducted in China revealed that the prevalence of depression, anxiety, and PTSD was estimated at 15.0%, 27.1%, and 9.8%, respectively due to the fear of contracting the virus themselves and death (19). Numerous studies are available that have shown how PTSD is currently on the rise due to COVID-19. There are other traumatic events occurring, but COVID-19 has caused a drastic increase in PTSD symptoms, especially in healthcare professionals. Having to care for patients with COVID-19 while trying to protect your own health and the health of your loved ones can evoke increased stress, anxiety, fear, and feelings of hopelessness in the daily work environment and at home. Some healthcare professionals have had to walk away from the profession they genuinely love.
For those who have decided to stay in the profession, the need for treatment is the main priority. Before a healthcare professional can help their patients, they must first care for themselves because without proper treatment, they may cause a cascade of tragic events to occur. There may be an increase in medication errors, possible patient abuse, neglect, or procedural mishaps.
Self Quiz
Ask yourself...
- How does Laura’s travel assignment impact her view of nursing and contribute to her feelings?
- Think about your work environment. How many travel nurses helped in the care of patients who had COVID-19?
Current Therapy
Post-Traumatic Stress Disorder (PTSD) will get worse without treatment. The Veterans Health Administration and Department of Defense (VA/DoD) and the American Psychological Association (APA) in 2017 each establish treatment guidelines for PTSD, which are recommended for treatment of PTSD (20). Current treatment strategies for control of trauma associated symptoms of PTSD have recently been updated by the Veterans Affairs (VA) and the Department of Defense (DoD) after over a decade of dedicated research (21). Both guidelines recommend the use of Prolong Exposure (PE), Cognitive Processing Therapy (CPT) and trauma focused Cognitive Behavioral Therapy (CBT).
The reason why there is strong support for these therapies is because these treatments are evidence-based and trauma-focused. This means they directly address the individual’s memories, feelings, and thoughts related to the traumatic event. These therapies are currently the gold standard for treatment. Eye Movement Desensitization and Reprocessing (EMDR) therapy is also trauma-focused therapy (20, 21). Non-trauma-focused treatments include medication and relaxation therapy.
Prolong Exposure
Prolonged exposure (PE) is strongly recommended by both the APA and VA/DoD as successful treatment for PTSD. Prolonged exposure is based on emotional processing theory which states that traumatic events are not processed emotionally at the time of the event. Theory goes on to suggest that fear is represented in the memory as a cognitive structure that includes representation of the feared stimuli, the meaning associated with the stimuli, and the responses to the stimuli. Prolonged exposure therapy consists of a patient being instructed by a therapist to confront traumatic memories and expose themselves continuously to fearful stimuli with the goal of reaching habituation or extinction.
Some therapists believe that prolonged exposure tends to activate higher rates of fear in individuals suffering with PTSD (21). Psychoeducation about PTSD and the various reactions to trauma, breathing retraining, and vivo and imaginal exposure (two types of exposure) are the main components of prolonged exposure therapy (20). In vivo exposure helps the patient with approaching situations, people, and places they have been avoiding because of the fear response that comes from the traumatic event. This is repeated until the distress decreases.
Imaginal exposure helps the patient to approach the memories, emotions, and thoughts surrounding the traumatic event that they have been avoiding. The patient recounts a narrative of the event in the present tense repeatedly while tape recording themselves as part of homework therapy. Then, the therapist and patient will process the information revealed during the imaginal exposure. This will allow the patient to activate their fear structure and incorporate new information. This process usually takes 8 to 15 sessions (20).
Cognitive Processing Therapy
Cognitive processing therapy (CPT) utilizes social cognition theory and the informed emotional processing theory. Following a traumatic event, usually a survivor attempts to make sense of what has happened and oftentimes it leads to distorted cognitions regarding themselves, the world, and others. According to CPT, people tend to integrate the traumatic event with prior schemas they often assimilate accommodate or over accommodate (20, 21). The main goal of CPT is to shift a person’s belief toward accommodation which is a result of altering their beliefs enough to accommodate a new learning (20, 21). Sessions usually take 12 weeks, and incorporate psychoeducation about the cognitive model and exploration of the patient’s conceptualization of the traumatic event (20, 21).
Cognitive Behavioral Therapy
Trauma -focused CBT is based on behavioral and cognitive models that draw from cognitive behavior theories which include Prolonged Exposure and CPT. The aim of this type of therapy is to modify negative appraisals, correct the auto biographical memory, and remove problematic behaviors and cognitive strategies. It is believed that guilt-associated appraisals tend to evoke negative effects and are usually paired with images and thoughts of the trauma. This causes repeated reconditioned memory of the trauma-producing distress leading to tendencies to suppress or avoid the trauma related stimuli (20, 21). The techniques associated with CBT include exposure and cognitive restructuring.
The exposure technique for a traumatic memory utilizes imaginal exposure, writing about the trauma. and reading the traumatic memory out loud. Treatment for a traumatic-related stimulus usually involves in vivo exposure or instructing patients to identify various triggers of re-experiencing (20). Patients are also taught to practice discrimination of “then verses now “(20). The most important part of cognitive restructuring is teaching patients to identify the various dysfunctional thoughts and erroneous thinking and replace them with rational alternative thoughts and reconsider beliefs about themselves, the trauma, and the world (20).
Eye Movement Desensitization and Reprocessing (EMDR) Therapy
Eye Movement Desensitization and Reprocessing (EMDR) is a type of traumatic exposure therapy in which healthcare professionals help the individual make their eyes move back and forth while they imagine the trauma. The EMDR therapy allows for the individual to reprocess the memory while addressing the past, present, and future aspects of the traumatic memory. EMDR can be used to help reduce anxiety and depression associated with PTSD. Therapists have indicated individuals who participated in therapy sessions twice daily (prolonged exposure session in the morning and an EMDR in the evening) were found to have higher satisfaction rates and reduced PTSD symptoms. EMDR has been shown to reduce fear and leave patients feeling relieved and satisfied (21).
Medication Therapy
The current medication therapy recommended by the American Psychological Association for PTSD treatment are paroxetine (Paxil), fluoxetine (Prozac) and venlafaxine (Effexor). Based on the most relevant and recent research, these medications have shown the most benefit as monotherapy in treatment of post-traumatic stress disorder symptomology (21). The relative benefit of using selective serotonin reuptake inhibitors (SSRI) or selective norepinephrine reuptake inhibitors (SNRI) is side effects profiles are generally well tolerated (21). All medications must be customized for everyone because people react differently to medications and their dosages.
Medications that help with PTSD symptoms may be in conjunction with antidepressants. These include:
Clonidine and Guanfacine, Risperidone for agitation
Clonidine, Prazosin and Trazodone for trauma related nightmares
Some beta-blockers (such as Propanol) to decrease hyperarousal symptoms, but it has not been approved by the FDA (21, 22).
Another medication therapy that has grown attention for treatment of PTSD is the Stellate Ganglion Block (SGB) injection. While SGB treatment has been around for a while to treat patients suffering with chronic pain and some neurological problems, it is now being used in the treatment of PTSD. Positive results include improving PTSD symptoms and reducing or eliminating suicidal ideations (23). The procedure is performed under local anesthetics placing the medication at the C6-C7 level guided by ultrasound or x-ray imaging. The injection resets the sympathetic nervous system to its pre-trauma state. The effects can be felt as early as 30 min after injection and can last for years. Research has shown that the overall success rate has averaged 85% - 90% range (23).
Relaxation Therapy
Relaxation therapy is a form of psychotherapy that utilizes breathing techniques, progressive muscle techniques, and meditation and to illicit a voluntary relaxation response of the individual. Sometimes the use of guided imagery is used to help the individual focus on positive mental images. This technique helps lower blood pressure, relieve muscle tension, and lower stress.
Progressive Muscle Relaxation has been used to help reduce fatigue in nurses and relieve PTSD symptoms. This technique involves sequential tensing of major muscles in the body which reduces feelings of tension and lowers perceived stress. Progressive muscle relaxation can be performed anywhere at any time. This technique can decrease the pulse rate, increase the individual’s oxygen saturation, and is sometimes used in conjunction with other forms of psychotherapy (24, 25).
Coping Mechanisms
For general individuals experiencing PTSD, it is sometimes difficult to cope with the mountain of symptoms that they may experience. For healthcare individuals experiencing PTSD it is critical that they seek treatment and develop coping mechanisms to deal with their symptoms because if they do not, their actions can become detrimental to their patients and themselves.
There are negative and positive coping mechanisms. Negative coping mechanisms include avoidance, becoming defensive and confrontational, displacement of feelings, suppression, self-isolation, and destructive behavior (25). There are three broad categories of coping responses. They include voluntarily seeking or receiving social support, voluntary strategies of gathering information and rehearsing responses to danger, and involuntary deployment of an unconscious homeostatic mechanism that reduces the disorganizing effects of sudden stresses (25, 26).
Healthcare professionals have resources available to help them cope with PTSD. Some workplaces have elicited the help of a psychiatrist or psychologist to provide drop-in services at the work site. Various positive coping mechanisms include:
- Spiritual guidance in prayer
- A strong support system to lean on such as a sponsor that the individual can call when feeling overwhelmed
- Including family in the healing process
- Performing mindful meditation (one of the newest forms of coping mechanisms for PTSD which encompasses a form of meditation in which the individual focuses on current sensations and feelings without applying any thoughts to them. This results in mental clarity and reduction of stress.
Moral resilience describes when an individual can confront distressful and uncertain situations with courage and confidence while relying on a strong system of values and beliefs. Moral resilience helps keep the individual “in check,” which allows their mind to conceptualize the situation, knowing when events are out of their own control. Moral resilience must be gradually built and developed by an individual and requires persistence and experience (26). Nurses should focus on developing moral resistance when caring for patients.
Other positive coping mechanisms include yoga, relaxation techniques, guided imagery to focus on positive thoughts when the stressors resurface, prescription medication for PTSD, peer support at work, professional counseling, group therapy, tai chi, and developing a hobby.
Self Quiz
Ask yourself...
- Which therapy option would you choose for Laura and her co-workers and why?
- Think of your work environment. Do you know what resources are available to you if you experience PTSD?
- How can you help your colleagues cope with the day-to-day pressures of working in a high stress environment?
- Think about the case study. Perform a complete assessment of Laura and her work situation and develop a plan of care for her and her co-workers.
Conclusion
Post-traumatic stress disorder can be a very debilitating condition. PTSD affects millions of people a year during non-pandemic crises. This condition nearly doubles during pandemic crises, especially for healthcare professionals. Healthcare professionals are the first line of help for the public. In order for them to do their jobs effectively, mental health must be a top priority. COVID-19 has caused an increased level of PTSD in healthcare professionals. As we watch colleagues, strangers, and loved ones battle with or succumb to COVID-19, we may find ourselves feeling hopeless and wanting to leave the profession we love.
Health care professionals develop a bond with their patients as well as their colleagues. It is that bond that gives some people more purpose than others and helps them to get through PTSD. Healthcare workers must receive the help that they need so that they can continue to help their patients.
Many organizations now offer counseling, time off, peer support, and incentives for healthcare professionals who engage in self-care. Proper treatment can alleviate or control PTSD in healthcare workers. Our goal in the future is to continue to make the physical health, spiritual health, and mental health of all healthcare workers top priority so we can continue to give the best care to everyone who comes to us for help.
Self Quiz
Ask yourself...
- Reviewing the phases listed above, think of how you would answer the following questions. What phase would you assign Laura?
- Laura was awakened by her neighbor screaming for everyone to get out of the apartment because there was a fire. Once outside Laura watched in horror as her belongings were burned in the flames. What phase is Laura experiencing?
- Laura is speaking with the Red Cross and her Agency regarding temporary placement. She was given permission to go back to the apartment to make a list of things she lost in the fire. What phase is Laura experiencing?
- Laura receives a call from her sister who tells Laura that she can come back home and stay with her and forget about the job. Laura breaks down in tears and tells her sister she feels so lost. What phase is Laura experiencing?
- Laura receives a settlement from the insurance company and asked her sister to come along with one of her previous neighbors to go shopping for a new apartment and new furniture to furnish the apartment. As Laura approaches the street of the old apartment complex, she gets an overwhelming feeling of depression and becomes quiet as she experiences a flashback of the night of the fire and quickly changes directions to another street. What phase is Laura experiencing?
End of Life Process
End of Life Process
Introduction
Have you ever cared for someone who was dying, known someone who was in hospice, or just wondered what happens as we die? What exactly does “end of life” refer to? End of life is a broad term, and its meaning can vary from person to person. End of life is a time when death is approaching, usually in a matter of days.
This occurs in various patients experiencing a variety of ailments including end stage cancer, dementia, chronic diseases, and someone who may have organ failure after an accident (3).
Oftentimes, caregivers have little to no experience in caring for a patient experiencing the end-of-life process and can easily find themselves feeling overwhelmed, confused, and burned out. Understanding what to expect during the final weeks and days of life is imperative to cope with the changes as they occur.
These changes can vary from person to person. Although patients progress through the end-of-life process differently, there is usually a recognizable pattern of decline that occurs. To provide the best possible care and prepare both the dying patient and their family members, it is important for the nurse and caregiver to be able to distinguish the phases of the end-of-life process: transitioning, actively dying, and final moments.
Transitioning
The transitioning phase, otherwise identified as the pre-active phase, usually signals that a person is approaching the last two-to-three weeks of their life. During this time, caregivers might start to notice obvious changes, an increase in sleeping, for example. A transitioning person can sleep upwards of twenty hours per day. This significant increase is part of an overarching decrease in the patient engaging with the world and day-to-day life.
Beyond sleeping, examples of this disengagement include interacting less with friends and family, less desire to do one’s usual activities, and a lack of interest in things that were once pleasurable. Additional signs of a patient transitioning include increased weakness and decreased mobility.
These changes typically include a decline in function, becoming non-ambulatory, chairbound, and ultimately, bedbound. Patients may begin to fall during this time. Progressively, the patient will become more dependent on their caregivers to assist them with activities of daily living (ADL), which include bathing, eating, transferring, toileting, and continence. They will likely become bedbound.
Another indicator that someone may be transitioning is a change in nutrition and intake. Eating and drinking less is an expected part of decline during this time. Many patients will report a lack of appetite, taste changes, and an overall lack of interest in food and liquids. Changes in swallowing may further complicate a person’s ability to eat and drink.
It is not uncommon to downgrade a person’s diet during the transition phase. This might include going from a regular diet, down to soft, and finally, to pureed. Liquids are usually given in small amounts and with an added thickener. These changes are necessary to prevent choking and aspiration. Fluid overload is a risk at this point and can detract from one’s comfort, cause swelling, or crackles in the lungs.
“Approximately 43% of all palliative patients are affected by terminal agitation, which can manifest as restlessness, sweating and patients’ statements as verbal or facial expressions and defensive reactions” (5).
Increased agitation, anxiety, and restlessness may also arise during the transitioning phase. Terminal agitation and terminal restlessness are both unique to the last week or so of someone’s life and are often caused by physiological changes that occur during the end-of-life process but can also be a result of medication or emotional changes. Even if the patient had been calm previously, it is important to note that these symptoms may still occur.
Signs of terminal agitation include an inability to remain still, picking at items in the surrounding environment, and increased confusion. Fortunately, there are medications that can be given at the end of life to promote comfort and stop these symptoms when they arise. Lastly, it is not uncommon for the transitioning patient to have visions of and talk to deceased friends and family – both are normal and could sometimes be interpreted as a welcoming sign from loved ones.
Self Quiz
Ask yourself...
- How long does the transitioning phase typically last?
- What is another name for the transitioning phase?
- How do people change while transitioning?
- What are some ways you could care for someone that is transitioning?
Active Dying
Following the transition phase, most patients will then enter the final phase of the end-of-life process, the active dying period. This precedes imminent death. It can be hard to determine precisely when this stage begins. This phase usually lasts only two to three days and showcases significant signs of patient decline that differ from the previous phase, including a decrease in alertness and responsiveness.
For example, a patient may go from a semi-comatose state to comatose or obtunded and minimal reaction should be expected (1). Their eyes may be open or shut, and there is little movement in all extremities. This period can be described as a deep sleep.
Caregivers often describe it as a time of waiting. Cognitive changes, in combination with the previous changes in swallowing, make the intake of food, liquids, and medications unsafe. The patient is at high risk for aspiration. Mouth swabs can be used to hydrate the oral cavity and to do mouth care.
Medications that are liquid or can dissolve under the tongue are safe and can be used to manage symptoms at the end of life. Hospice patients are provided a comfort kit of medications to use should symptoms arise.
Additionally, changes in vitals are expected during this phase, and they typically do not cause the patient any discomfort. For example, temperature fluctuation is common at the end of life. It is not abnormal to have an elevated temperature during the active dying phase. This can be remedied with cooling measures such as a cool towel on the forehead or a fan to cool down the room. The skin may feel clammy as well.
Following, changes in blood pressure and heart rate may also occur. Blood pressure begins to trend lower during the pre-active phase and can become very low during the last few days of life. The heart rate will usually trend upward and can be well over 100 beats per minute, however, this is just something for the hospice nurse to note and is not usually treated.
Symptom management at the end of life can be difficult. Failure to adequately control symptoms can have a negative impact on one’s quality of life. These symptoms may include pain, respiratory distress, GI issues, and mobility changes (2). Pain while dying is one of the most common areas of concern for someone who is actively dying, and of course, no one wants to see their loved one in pain during their final days of life. The body becomes very sensitive to the slightest movement or touch, which can present challenges for caregivers when considering that the patient still needs to be cleaned, changed, and repositioned.
When the patient is no longer verbalizing their comfort, verbal pain cues must be assessed. These include grimacing, a furrowed brow, frowning, and possibly moaning. In some cases, repositioning can be an effective pain-relieving measure. Thankfully, pain can be treated up until death occurs.
Opioids are commonly used in end-of-life care, due to their ability to effectively manage pain without hastening death. Morphine is an example of a commonly used opioid (4). Nonpharmacological measures can also be used to relieve pain. This may include things like repositioning and soothing music.
Decreased urination is also common during the active dying phase. This is completely normal and expected. Caregivers may find that they do not need to change diapers as often. Urine may also appear darker in color, appearing a deep amber color due to more concentrated urine.
Excessive secretions can lead to something commonly known as the “death rattle.” This term is almost synonymous with the last days of life. It can be described as a moist sound that is audible when someone breathes and is a good indicator that death is near. The secretions collect in the throat due to a lack of coughing and the inability to clear them out (8).
Turning the patient on his or her side may help the secretions drain, and there are medications that can be administered to help dry them out. It is important to note that not everyone will experience this, and by the time it occurs, there is a disconnect within the patient, and he or she is not likely to experience any discomfort.
Maintaining skin integrity and preventing pressure injuries is also an important consideration during this time. With all the other previously mentioned changes occurring, it can be hard to provide the attention that the skin requires. Like other organs, the skin begins to fail in an actively dying patient (9).
This does not necessarily mean that pressure injuries and skin breakdown are inevitable. It is important to consider goals of care during this time. An aggressive approach to preventing skin breakdown might not be what the patient wants or necessarily needs. Measures for pressure injury prevention might include repositioning, use of pillows for elevation, hygiene, and moisture management.
Self Quiz
Ask yourself...
- How long does the active dying phase usually last?
- How is active dying different from transitioning?
- What are some commonly experienced changes during this time>
- Have you cared for someone during this time? What did you find to be most challenging?
Final Moments
It can be hard to imagine the final moments of someone’s life. This is especially true for caregivers and families who have witnessed steady decline throughout both stages of dying. There are likely to be signs that death is possible at any moment. A patient can be expected to be comatose with little to no response when death is imminent. The obtunded patient appears to be in a deep sleep. They are no longer verbally or physically responsive to voice or tactile stimulation.
In addition to changes in vitals described previously, changes in respiration usually occur. This is typically the most obvious change. Patterns can vary from shallow and fast to deep and slow. Periods of apnea are also normal. Cheyne-stokes breathing may also be present (3).
Skin changes are also expected; pallor, cyanosis, and mottling are signs that death is near. The body may begin to feel cool, especially in the hands and feet. Comfort medications can still safely be used up until death occurs. As mentioned before, foods and liquids should not be given at this point. Caregivers should continue to talk to the patient, as their hearing will remain until the end.
Hospice
Most people wish to die peacefully at home. Unfortunately, for many, this is not the case. Over 30% of people die in a hospital setting (6). Hospice is a form of palliative care and involves caring for the terminally ill as they begin the end-of-life process. A terminally ill patient has a life expectancy of 6 months or less. This is a comfort focused approach to care. The natural process of dying is accepted and allowed to proceed.
No life prolonging treatments or procedures are elected. Choosing a hospice allows both patients and their caregivers to achieve their end-of-life care goals. Hospice care includes an interdisciplinary team composed of nurses, physicians, aides, chaplains, and social workers. It includes symptom management, and emotional and spiritual support. There is also a bereavement team that is available after death. Medicare part A covers hospice services nearly completely.
Hospice care can be a short or long journey, with many ups and downs. For some, the prognosis might be obvious, but for others, it might be filled with many questions and much uncertainty. The benefits of hospice care are proven and can lead to a peaceful death. “The main care focus for patients is symptom management, which improves the quality of the remainder of their life.
Palliative care involves not only the patient but also their family members. Other measures are also taken so that the patients can live life comfortably and maintain dignity” (7). Both caregivers and patients seek to understand what end of life care entails and how to maintain comfort at end of life. Hospice clinicians should spend time providing education on this process to all of those involved.
Spiritual Considerations at End of Life
Taking care of the dying should be looked at from a holistic point of view. Addressing the physical needs of someone who is dying while ignoring any spiritual needs would be doing a disservice. Spirituality is considered the meaning of life. It may include religion, beliefs, or family traditions. It can mean different things to different people.
During end-of-life care, it has been shown to be disrupted in patients. Spiritual needs tend to be greater at the end of life. It is also frequently overlooked by healthcare professionals (10). Palliative care workers can help address spiritual needs in their patients by showing compassion, humility, and openness.
Dying patients may be conflicted spiritually due to things like guilt and unresolved issues. When spirituality is addressed appropriately, patients can more positively cope with illness. Caregivers of the dying should be aware of the relationship between a terminal prognosis and unmet spiritual needs.
Self Quiz
Ask yourself...
- Have you been present when someone died? How did it make you feel to witness this?
- What are signs that death is imminent?
- How do respirations change just prior to death?
- What education would you provide to a caregiver during this time?
Conclusion
Hopefully, this has been an informative piece and a guide on what to expect during end-of-life care. No two people experience death and dying in the same manner, and it can be challenging both physically and emotionally during the end of life. Proper symptom management during this time is crucial in ensuring that one dies comfortably. One should also consider any unmet spiritual needs and how, if unaddressed, could lead to poor patient outcomes.
Palliative care at the end of life can be a great help for caregivers. Hospice can be a great resource in managing symptoms and providing support up until death and beyond. Most people do not have experience in caring for a dying person and need education and assistance throughout the journey. Not everyone who is dying will experience all the symptoms mentioned in this course, and it is important to note that everyone experiences the end-of-life process in their own way and at their own pace.
Sexual Harassment Prevention
Introduction
Sexual harassment is a serious issue within the healthcare workplace. One systematic review research study found that sexual harassment rates against female nurses was as high as approximately 43% (5). According to an article published in the American Journal of Critical Care in 2021, recent studies estimate around 60% of female nurses and 30% of male nurses have reported sexual harassment (3).
For both student and registered nurses, patients were the most likely perpetrators. However, this varies, and some research suggests that physicians and patient relatives were also at an increased likelihood of being perpetrators of sexual harassment toward registered nurses (8). It is important to remember that sexual harassment is not limited to female registered nurses; male nurses are also at risk of experiencing sexual harassment in the workplace.
The impacts of sexual harassment affect nurses in many negative ways. There are obvious psychological consequences, but there is also evidence to suggest that work performance and productivity can also be negatively affected (12). Many states have recognized the significant impact of this issue and have taken measures to empower nurses to prevent and/or address sexual harassment.
What Is Sexual Harassment?
Sexual harassment is commonly thought to be unwelcome contact. However, sexual harassment takes many forms. It can be defined as unwelcome sexual behaviors or actions which may be verbal, physical, mental, or visual (13).
Listed below are some common examples of potential sexual harassment:
- Actual or attempted rape or sexual assault
- Pressure for sexual favors
- Deliberate touching, leaning over, or cornering
- Sexual looks or gestures
- Letters, telephone calls, personal e-mails, texts, or other materials of a sexual nature
- Pressure for dates
- Sexual teasing, jokes, remarks, or questions
- Referring to an adult as “girl,” “hunk,” “doll.” “babe,” “honey,” or other similar terms
- Whistling at someone
- Turning work discussions to sexual topics
- Asking about sexual fantasies, preferences, or history
- Sexual comments, innuendos, or sexual stories
- Sexual comments about a person’s clothing, anatomy, or looks
- Kissing sounds, howling, and smacking lips
- Telling lies or spreading rumors about a person’s sex life
- Neck and/or shoulder massage
- Touching an employee’s clothing, hair, or body (4, 13)
The U.S. Equal Employment Opportunity Commission defines sexual harassment as “unwelcome sexual advances, requests for sexual favors, and other verbal or physical harassment of a sexual nature.” Sexual harassment can also include offensive remarks about an individual’s gender or sexual orientation. No matter the type or amount of harassment, it can disrupt the workplace and potentially create a hostile work environment (10,11) As you can see, the definition of sexual harassment is broad and can encompass many situations.
Self Quiz
Ask yourself...
- Many nurses do not know that the definition of sexual harassment is broad. Knowing this, are there any situations you would consider sexual harassment, where you previously would not have?
Why Are Nurses Vulnerable to Sexual Harassment?
Nurses are vulnerable to sexual harassment by the very nature of their position. The role of nursing surpasses many societal norms regarding physical contact and involves intimate care of patients both physically and emotionally. This role is often exploited by perpetrators – they may take advantage of a nurse’s position and caring demeanor as a means to harass them (8).
Staff-on-staff harassment is also commonly reported by nurses (8). Nurses are potentially predisposed to this type of harassment due to their subservient position to many staff members (physicians, administration) and the subsequent power imbalance that results.
Self Quiz
Ask yourself...
- What workplace environmental factors can lead to nurses experiencing sexual harassment?
Key Points for Sexual Harassment
Sexual misconduct vs. sexual harassment – Sexual misconduct is a type of sexual harassment. Sexual behavior can turn into sexual harassment when the recipient receives the behavior in an unwelcome manner. The term “unwelcome” refers to unsolicited or uninvited behavior and undesirable or offensive behavior (11).
Females and males can both be victims – Any unwelcome sexual behavior may be considered sexual harassment, regardless of the gender of the perpetrator and recipient. Male-on-male, female-on-female, female-on-male, and male-on-female types of harassment may occur (11).
Sexual harassment can affect witnesses – Anyone who is affected by the sexually offensive conduct may be a victim. This may include a person witnessing or overhearing sexually-harassing behavior (1).
It can occur outside the working environment – The “working environment” is not limited to the physical location of work. A “working environment” may be extended to any location where work occurs, such as remote locations, off-site locations, and temporary working locations (1, 11).
It doesn’t only occur in person – Sexual harassment can occur on and off the clock. It can occur physically and virtually. Unwelcome sexual conduct through email, phone calls, texts, social media postings, and other mediums may constitute sexual harassment (6).
Two Types of Sexual Harassment
- Quid pro quo – Quid pro quo means “a favor for a favor.” In this sense, it refers to an authority figure (manager or supervisor) requesting a sexual favor in exchange for preferential treatment. This could be in the form of a promotion, raise, preferred assignment, or any other job benefit which they may affect (7).
- Hostile work environment – Another method by which an individual may coerce sexual favors is through the threat or actuality of a hostile work environment. This refers to creating or threatening to create an intimidating, hostile, or offensive work environment in order to influence sexual favors or behavior (7).
Self Quiz
Ask yourself...
- What would be an example of quid pro quo?
- How is this type of harassment different than hostile work environment?
What Should Nurses Do If They Experience Sexual Harassment?
If you feel you have been the victim of unwelcome sexual behavior (sexual harassment) there are avenues available to you for support and to report the behavior.
- While it may not be an easy thing to do (or even possible), try to make it known that the sexual behavior is unwelcome and unwanted. It is your right to inform the person of your stance and to demand the behavior cease. Though this can be difficult and uncomfortable, it is often the most effective method (2). If you decide to confront the perpetrator, try to remain calm and de-escalate the situation as much as possible.
- You should be explicit in explaining the behaviors that are unwelcome so that the perpetrator can fully understand his/her actions. If you are uncomfortable confronting the perpetrator, consider confiding in a close friend, coworker, or supervisor who can accompany you or advise you on the next steps.
- Another way is to interrupt the harasser to distract them from the situation (2)
- Next, make sure to document the scenario. Write down all of the details that you can recall; including any witnesses. This can be helpful in the future.
- Reporting the issue through the appropriate channels is the next step. Oftentimes, this involves speaking with your supervisor and someone in human resources. While discussing the situation, do not make excuses for the perpetrator or try to “shrug it off.”
How or whether you report sexual harassment is a personal choice, and you are not limited. However, you should strongly consider reporting the incident because it could escalate further in the future. The perpetrator may also be sexually harassing others. Every workplace should be free from sexual harassment and many states have laws protecting nurses against workplace sexual harassment, including harassment received from patients and family members. There are several options for reporting sexual harassment, and there are several nuances with jurisdiction and handling of complaints. However, you should not be discouraged from reporting through the appropriate avenues.
1. Within your organization.
You may contact your supervisor or human resources representative to report an incident. This is often a more comfortable route for nurses as they may be familiar with these individuals. Your organization should have policies and procedures for handling sexual harassment reports which may include escalation to law enforcement as necessary. This is often the fastest method for reporting. Remember that reporting to your supervisor, ethics officer, or human resources official does not preclude you from reporting to other agencies as appropriate. If you wish to remain anonymous, check with your organization to see if they have a policy that gives you that option.
2. Law enforcement.
Criminal incidents of sexual harassment may be reported to law enforcement as appropriate. Oftentimes your human resource officer can assist in determining if this is necessary or required by state law. If you ever feel that your physical safety is threatened, do not hesitate to contact law enforcement.
3. Office of Executive Inspector General (state government employees).
State employees may file a report directly with the OEG. To initiate a report, it is best to contact your ethics officer for guidance.
4. U.S. Equal Employment Opportunity Commission (EOCC).
Sexual harassment is a violation of section 703 VII. The EOCC is charged with administering this statute and provides another option of relief for those who have experienced sexual harassment. The statute for reporting an offense to the EOCC is 180 days from the date of the incident. Of note, the EOCC may hold employers responsible for taking all steps to create an environment free of sexual harassment and can offer an additional avenue for support. This law may be extended up to 300 days depending in the state laws surrounding sexual harassment (10).
Self Quiz
Ask yourself...
- How would you handle sexual harassment differently knowing your rights and reporting avenues?
- Are there any previous situation you would have handled differently?
Whistleblower Protections
Retaliation for reporting sexual harassment is illegal under both federal and state statutes. The U.S. Equal Employment Opportunity Commission prohibits retaliation aimed at employees who assert their rights to be free of harassment (9).
Concluding Points
- Sexual harassment can take place in many venues and formats. It is broadly defined as any unwanted or unwelcome sexual behavior or advances.
- Sexual harassment is experienced frequently by nursing professionals due to the nature of their positions.
- You have a right per federal and state laws to be free of sexual harassment in the workplace.
- If you experience sexual harassment, you should tell the harasser to stop and report the incident in one of the various methods listed above. Do not forget to document provide a thorough report of the incident.
- You have a right to report sexual harassment without retaliation per federal laws.
Following a DNR: An Ethical Dilemma in Nursing
Introduction
End-of-life issues are often full of emotion and difficult to deal with for all involved. Do-not-resuscitate (DNR) orders can present many moral and ethical dilemmas in nursing. It takes the entire healthcare team, including the patient and their family, to ensure that all final wishes for the patient are followed. In order to understand this ethical dilemma in nursing, we must first define what ethical dilemmas are and what a DNR order is.
Nursing Ethics/Ethical Dilemma
Ethics are a system of moral principles or rules of conduct recognized by a particular group. However, the American Nurses Association (ANA) has developed its own code of ethics. The ANA Code of Ethics with Interpretive Statements includes nine provisions that direct a nurse’s moral and ethical practice. It reads:
Provision 1: The nurse practices with compassion and respect for the inherent dignity, worth, and unique attributes of every person.
Provision 2: The nurse's primary commitment is to the patient, whether an individual, family, group, community, or population.
Provision 3: The nurse promotes, advocates for, and protects the rights, health, and safety of the patient.
Provision 4: The nurse has authority, accountability, and responsibility for nursing practice; makes decisions; and takes action consistent with the obligation to provide optimal patient care.
Provision 5: The nurse owes the same duties to self as to others, including the responsibility to promote health and safety, preserve wholeness of character and integrity, maintain competence, and continue personal and professional growth.
Provision 6: The nurse, through individual and collective effort, establishes, maintains, and improves the ethical environment of the work setting and conditions of employment that are conducive to safe, quality health care.
Provision 7: The nurse, in all roles and settings, advances the profession through research and scholarly inquiry, professional standards development, and the generation of both nursing and health policy.
Provision 8: The nurse collaborates with other health professionals and the public to protect human rights, promote health diplomacy, and reduce health disparities.
Provision 9: The profession of nursing, collectively through its professional organizations, must articulate nursing values, maintain the integrity of the profession, and integrate principles of social justice into nursing and health policy.
An ethical dilemma in nursing arises when decisions are made that go against the ANA Code of Ethics with Interpretive Statements.
It is important to note that the nurse's main duty is to be an advocate for their patient, meaning that all actions should be in the patient’s best interest. Adhering to this principle will ensure a clear moral path where ethical dilemmas in nursing can be avoided (1).
Self Quiz
Ask yourself...
- What are ethics?
- How many provisions are in the ANA Code of Ethics?
- State 3 provisions of the ANA Code of Ethics.
- What is an ethical dilemma?
DNR
A DNR order is a situation where, should the patient's health deteriorate and progress to cardiac arrest, the healthcare team will not provide cardiopulmonary resuscitation (CPR). The physician usually gives this order after consulting with the patient and family. Should the patient be unable to make decisions about their health, their designated power of attorney (POA) for healthcare decisions will be able to make that determination.
The DNR order is usually reserved for patients who are gravely or terminally ill and have a strong possibility of dying during their stay at the hospital. Once the DNR is ordered, it will stay in effect until the patient passes, leaves the hospital, or rescinds the order (3, 5).
Self Quiz
Ask yourself...
- What does DNR stand for?
- What type of patient would typically have a DNR order?
- How long is the DNR order in effect?
- What is CPR?
Possible Ethical Dilemmas with a DNR
There are different situations where a DNR order could pose an ethical dilemma for the nurse. All of these examples involve the nurse's feelings, beliefs, or morals contrasting against the DNR order or the circumstances leading to the DNR order.
- Operating Room/Procedural Suite: In many facilities and healthcare systems, when a patient is undergoing surgical intervention, the DNR is suspended while the patient is in the surgical suite. The consent form for the procedure will indicate that the DNR order will be suspended, and the patient/family must agree to this to proceed with the operation.
- Should something happen during the procedure/operation, is it right to suspend the patient's DNR wishes? The hospital has metrics, including operating room mortality, that they must keep low. Suspending the DNR gives the facility a better opportunity to meet these metrics. These metric results can be viewed and compared from hospital to hospital.
- Further, a DNR order can create confusion among the surgical team. Each member may have a different idea of precisely what the DNR means. Some team members may not even believe surgery should occur, given that the patient has a DNR order. In particular, the anesthesiologist may face an ethical dilemma when providing anesthesia to a patient with a DNR order. The anesthesia can cause cardiopulmonary arrest; if the anesthesia causes such, does treating the anesthesia-induced arrest go against the DNR order (4)?
- Suffering: Another dilemma regarding a DNR order is the idea of patient suffering. It is tough to quantify and qualify suffering. That being said, one of the nurse's prime responsibilities regarding their patients is to relieve suffering. No nurse anywhere likes to see their patient in pain and suffering. In their attempts to help reduce that suffering, the nurse may push the patient or the patient's family into considering a DNR order even when it may be inappropriate given the patient's diagnosis and prognosis.
- This thought could extend to the nurse asking the physician to consult hospice services. It must be clear that not every patient who is suffering should have a DNR order; unfortunately, pain and suffering sometimes go hand-in-hand with recovery.
- There are also many different types of suffering: physical, emotional, mental, spiritual, etc. Is it right to initiate a DNR order based on these types of suffering alone? Who can say what suffering is, especially when it can't be seen (6)?
- Religion: Another factor that can impact the ethics of a DNR is the religious beliefs of the patient/family as well as the beliefs of the nurse.
- Some religions do not condone the idea of a DNR. This may stem from an erroneous understanding that the DNR is somehow assisting or facilitating death. This is not the case. A DNR means that no heroic measures will be taken should the patient stop breathing or should their heart stop beating.
- Yet, the stigma remains. There have also been cases where, when the prognosis was poor and the patient had deteriorated, a DNR was put into place. Later, the family reversed the DNR as they believed a miracle could happen and wanted to give time for their deity to move. Now, the family may be at odds with the healthcare team. One knows that God can perform a miracle and save the patient, and the other knows that the end is inevitable.
- The nurse's religious beliefs can also play a part. The nurse may believe that the DNR is premature and that the patient should still fight for life. Maybe the patient is a young one or someone who seems to have much to live for and should not give up. This nurse may find it hard just to let the patient go and could call a Code Blue despite the DNR order (2, 6).
- Capacity: The nurse needs to assess the patient's ability to make decisions for themselves, especially when a patient's faculties may come into question at the end of life. The decision for DNR is not one to be taken lightly; it is a life-or-death decision. The patient must understand what it means to be DNR, how it will affect the care plan, and what it means for their family and loved ones. Allowing the patient to make such a decision based on their condition, though their faculties may be compromised, could become an ethical dilemma (6).
- Effects on treatment: It must be noted that DNR means do not renew, not do not treat. That being said, the perception of the care that should be provided to a patient with a DNR order decreases dramatically. The idea that a DNR patient should have any procedure or operation is often scoffed at. This is especially evident when it comes to procedures meant to provide comfort but also have life-prolonging results.
- Procedures such as placing a gastrostomy tube to deliver parenteral nutrition may be needed for patient comfort and health but could be perceived as contrary to the DNR order. Also, nurses are far less likely to call a "rapid response" on a DNR patient if their condition begins to deteriorate; the nurse may not even call the physician until the patient passes because the DNR was in place. The patient should be treated as any other patient until the parameters of the DNR order are met. Nurses need to be aware of their own biases regarding DNR. Treatment should not be withheld or altered because of the DNR (2, 5, 6).
Self Quiz
Ask yourself...
- Name two possible types of ethical dilemmas concerning DNR.
- Why is a DNR order suspended when a patient undergoes surgery?
- How may a DNR order confuse the surgical team?
- Should all suffering patients have a DNR order?
How to Avoid Ethical Dilemmas with DNR
All parties agree that the best way to avoid any ethical dilemma regarding a DNR order is to have clear communication. Patients need to communicate their wishes to all their immediate family members. This will keep everyone on the same page and inform them about the patient's desires. Their end-of-life wishes need to be clear and without any confusion. In this way, the patient's wishes can be met despite what the family may believe.
It would be well advised for patients approaching the end of life to appoint a medical power of attorney who will ensure that all their expectations are followed. The decision for a DNR order must also be communicated to the healthcare team. It may not be enough to speak about the desire for the DNR, but also the expectations of their healthcare needs leading up to death as well.
The patient, their family, and the healthcare team must all understand what DNR means when it comes into play and how it will impact their care. Everyone involved in the patient's care must agree with the care plan, including the DNR. The patient and family should be educated about their diagnosis, disease process, prognosis, and treatments. In other words, a decision to have a DNR order must be made in advance.
If nurses are unable to reconcile the DNR decision within themselves even after discussing the issues with the healthcare team, they may need to step away from the situation (5).
Screening for Suicide Risk Factors in Pediatrics
Introduction
Our youth are our future, and their welfare (physical as well as psychological) is a public health concern. In the youth population, suicide is attributed as the 2nd leading cause of death (3). Moreover, suicidal ideations and attempts are even more common than suicidal deaths (3). Our youth's mental health must be addressed when conducting routine or urgent health screenings to deal with this global public health problem. Consequently, screenings for suicide risk factors in pediatrics have proven beneficial in suicide prevention, and most clinical practices have incorporated them into clinical pathways (3). Ultimately, screenings for suicide risk factors are vital tools that can be utilized to detect behaviors relevant to suicide. The results of those tools can serve as guides for warranted intervention.
The Significance of Screening Tools for Suicide Risk Factors in Pediatrics
The importance of screening tools for suicide risk factors in the pediatric population is evident. Screening is a fast and efficient method of identifying someone needing further evaluation (6). Those with positive findings on a suicide risk screening tool should be followed up with an assessment for suicide (6).
Screening for suicide in the pediatric population is essential. It is also necessary that the tools used are evidence-based for this specific population. The Ask Suicide Screening Questions (ASQ) is an evidence-based suicide risk screening tool used for medical and behavioral health pediatric patients (5). This is a frequently used tool that is approved by The Joint Commission (5).
There is a youth version of the ASQ that is developmentally appropriate for assessing suicide risk in children eight years of age and older (3). More importantly, the ASQ is available in multiple languages. Unfortunately, there are no screening tools for children less than eight years of age; therefore, a full mental health evaluation is conducted (3). Regardless of the approach selected, children are screened without their parents or guardians present for accurate results (3). Additionally, policies or plans of action must be in place if screenings or evaluations indicate positive results (3).
Self Quiz
Ask yourself...
-
As a clinician, how can you incorporate screening tools for suicide risk factors into your assessments?
Suicide Risk Factors in Pediatric Populations
In the past two decades, the suicide rate for adolescents has increased (4). Males continue to have a higher suicide death rate. However this rate has doubled for females during this period (4). The suicide death rate has tripled for those 12-14 years of age (4). Compared to the adult population, suicidal ideation, self-harm, and suicide attempts are now more common among the younger population (4). Contributing factors to this increase in suicide are (4).
- Bullying
- Social isolation
- Increase in technology and social media
- Increase in mental health disorders
- Economic recession
Statistics indicate that certain racial and ethnic minority youth experience higher rates of suicidal behaviors. American Indians and Alaska Natives have the highest reported rates of suicide attempts and ideation (4). There has also been an increase in suicide attempts among the African American youth (4). Risk factors that contribute to this include (4).
- Access to mental health services
- Poverty
- Historical trauma
- Adverse childhood experiences
In addition, the prevelance of suicidal thoughts and behaviors has significantly increased among the LGBTQ+ youth (4). Risk factors unique to this population include(4).
- Discrimination
- Violence and trauma
- Rejection
- Increased mental health disorders
While death by suicide is uncommon among children under eight years of age, factors such as anxiety, depression, or suicidal ideation can be present in this age group. (2) Research also indicates that racial disparities in children under 12 exist (2). Black children are twice as likely to die by suicide than white children (2).
There are specific warning signs of suicide risk for this age group that include (2).
- Verbalizing wanting to die or kill oneself.
- Displaying actions of hurting oneself.
- Engaging in self-harming behavior.
- Impulsive aggression.
- Giving away toys or possessions.
Genetics and history of suicide attempts are other factors to consider. One of the strongest predictors of completed suicides is a previous suicide attempt(4). Even more troubling is that risk significantly increases when there is family history of suicide (4).
As clinicians, we must maintain accountability for screening and assessing for all indicators of suicide potential. In saying that, environmental factors such as dysfunctional family dynamics, domestic violence, abuse and neglect, bullying, stressors (i.e., life-changing events or losses), and socioeconomic strains should be considered notable suicide risk factors that are highly impactful (4). Also, it is important to inquire about an individual's access to lethal methods, especially if they imply that they have a plan (7).
The psychological/physical health factors highly linked to suicide include (4,7).
- Depression or other mental health disorders
- Traumatic brain injury or concussion
- Chronic physical condition
- Alcohol or substance use/abuse
- Lack of social interaction or support
- Learning difficulties or disabilities
- Aggressive or disruptive behavior
- Excessive video game or internet use (more than five hours daily)
- In foster care or adopted
- Sexual orientation
- Impulsivity
Self Quiz
Ask yourself...
-
What are some risk factors that indicate immediate interprofessional collaboration?
-
How can you, as a clinician, better assess for suicide risks and identify patients who need prompt interventions?
Signs and Symptoms Associated with Suicide
There is no doubt that suicide among youth is a serious problem. Often, suicide signs and symptoms are comparable to those noted in depressive situations, and it is a fact that the majority of adolescents and children who attempt suicide do have mental health disorders (8). Most frequently, this is depression (8).
Some of the signs and symptoms linked to suicidal behavior include (4,7).
- Isolation from others
- Hopelessness
- Ridding self of cherished possessions
- Discussions of death
- Irritability or agitation
- Defiance
- Expressions of guilt or shame
- Violent behavior
- Personality changes
- Neglecting personal appearance
- Physical complaints
- Loss of pleasure in usual activities
- Low self-esteem
- Psychosis
- Changes in eating habits
- Changes in sleeping habits
- Feelings of sadness
Self Quiz
Ask yourself...
-
What signs and symptoms would indicate immediate intervention, even without initially using a screening tool?
Interventions for Concerns Related to Suicide Risk Factors
The ASQ outlines "Next Steps" to take in circumstances of positive results (3). This is based on a "Yes" response to any of the four questions, which would then prompt asking the fifth question. If the answer to question #5 is "Yes," the screening is marked as an acute positive screening, and the patient is considered at imminent risk. In that regard, the patient requires an immediate safety/full mental health evaluation; he/she must remain supervised in the clinical setting until safety is evaluated. At the same time, the environment is freed of harmful objects, and his/her physician or responsible clinician is notified (3).
Contrarily, if the answer to question #5 is "No," the screening is noted as a non-acute positive screen that insinuates a potential risk identified. The patient must remain in the clinical setting until his/her safety is evaluated. For that matter, there is a brief suicide safety assessment conducted to establish whether a full mental health evaluation is necessary (3). The clinician responsible for the patient's care or his/her assigned physician is also notified in this case (3). Essentially, the patient's safety is a priority.
Self Quiz
Ask yourself...
Think about your current practice.
- Are there guidelines in place for dealing with patients who are suicidal?
- How often are those guidelines or policies reviewed to assure appropriate practices are being implemented?
Management of the Suicidal Patient
Assessment and management of a suicidal patient is pertinent to prognosis. Although no intervention is 100% guaranteed to stop an individual from carrying out an act, interventions have proven to be positively impactful in many cases. It has been proven that asking questions pertaining to suicide risk does not increase an individual's likelihood of committing suicide (6). Rest assured that detailed assessments and evaluations facilitate deriving the most appropriate plans of care and should be included in the treatment approach.
Therefore, the following should be considered when managing suicidal behavior in pediatric patients (4).
- Assess for suicidal risk factors.;
- Assess mental status.
- Involve parents or guardians, if possible.
- Offer psychological education.
- Consider the need to hospitalize the patient.
- Interprofessional collaboration or involvement of other services (e.g., psychologist or psychiatrist, counselor, or crisis assessment team/public mental health service).
- Create a youth safety plan or make a referral to a mental health clinician with this expertise.
- Focus on treating underlying mental health problems with psychotropic medication (i.e. antidepressants).
- Psychotherapy.
- Cognitive Behavior Therapy (CBT).
- Dialectical Behavior Therapy (DBT).
- Document the risk assessment, interventions, and patient status.
- Promotion of continuity of care.
- Connect to resources. (2).
As previously mentioned, safety is a priority; hence, safety planning is an important evidence-based treatment approach. Research supports that those who participate in safety planning are less likely to experience suicidal behavior and more likely to seek mental health services (4). The safety plan consists of a list of coping strategie and sources of support and should encompass the following components (9).
- Recognizing signs of patient status worsening.
- Iidentifying and listing personal coping mechanisms.;
- Uutilizing family and friends as distractions from suicidal ideations.
- Iinvolving the family in problem-solving during a crisis.
- Ccontacting mental health clinicians and restricting access to lethal means.
Likewise, providing access to a resource such as the National Suicide Prevention Lifeline to patients and families is also a means for them to receive counseling, suicide educational materials, and referrals (1).
Self Quiz
Ask yourself...
-
Are you competent in assessing and intervening when faced with a patient who is at risk for suicide?
-
What do you believe is the best approach for making sure patients receive appropriate care and follow-up?
Case Study
A 12-year-old boy is brought to the ED via emergency transport after being found lethargic on the floor of his bathroom with an empty bottle of hydrocodone located close by his hand. It is assumed that he ingested an indefinite amount of hydrocodone tabs. His initial vital signs are temperature, 97.9 F; heart rate, 50 beats/min; blood pressure, 85/57 mm Hg; respiratory rate, 8 breaths/min; and oxygen saturation 95% on room air.
The patient is difficult to arouse, and Narcan is administered per protocol. Once the patient's condition is stabilized, he voiced his reason for the suicide attempt, which revolved around him being bullied by peers on almost a daily basis for the last couple of months. The patient excels academically and was a member of his middle school basketball team, which helped him cope until the season recently ended.
Additionally, the patient lives with his grandparents, and he stated, "Everyone is always making fun of how I dress and the car that my granddad drives. I'm just tired of people bothering me, and I wanted it to be all over." This was the patient's first suicidal attempt. During the one-on-one evaluation, it is noted that the patient made minimal eye contact and intermittently placed his head in his hands. You consider the appropriate next steps with the patient's safety of utmost importance. What next steps would you implement for managing this patient's care?
Self Quiz
Ask yourself...
- What next steps would you implement for managing this patient's care?
Recommendations
Conduct suicide assessments and evaluations on every visit because each visit affords the opportunity to identify, educate, and intervene. Research best practices and stay cognizant regarding recommendations for effective approaches associated with suicidal patients. Involve family members, other health care providers, and support personnel for a collaborative approach to meeting the patient's needs. Remember, inquiring about a patient's suicide risk does not increase his/her likelihood of engaging in suicidal behavior but rather serves as a vital means for intervening as opposed to neglecting to address the situation.
Human Trafficking
Human trafficking is a significant humanitarian issue in the United States and the world that has continued to grow in the past several years despite government and public efforts to combat it. With increasing news coverage of high-profile human and sex trafficking cases, the problem was recently brought into the American public’s eye. However, the results published by the Polaris Project make it evident that human trafficking is not just a problem of the elite or occurring in poorer areas. It is within our own neighborhoods and workplaces.
For healthcare workers in the United States, the war on human trafficking will be won through: gaining the knowledge to recognize the warning signs and specific characteristics of a potential trafficking victim; the most effective ways to intervene, which will enable the victims to gain access to help; and where to garner additional support in addressing the issue.
Prevalence and Definition
The Polaris Project estimates that collectively there are over 25 million victims of human trafficking worldwide. These are individuals that have been forced into sexual or labor servitude. Of those, approximately 48,326 were related to individual trafficking contacts in the United States (7). These numbers exemplify the number of potential victims that are not reaching out for help.
Often, when human trafficking is discussed, a common misconception is that it is simply the transporting of humans. Human trafficking covers a much broader scope than this. It is this a modern age form of slavery and involves the exploitation of individuals for monetary or sexual gain. As stated by the Department of Homeland Security, “Human trafficking involves the use of force, fraud, or coercion to obtain some type of labor or commercial sex act”(3).
As defined by U.S. law, there are three categories of human trafficking (all from 1):
- Children under the age of 18 induced into commercial sex
- Adults (age 18 or over) induced into commercial sex through force, fraud, or coercion
- Children and adults induced to perform labor or services through force, fraud, or coercion
The majority of trafficking in the United States involves sex crimes, followed by labor (4). These crimes may be occurring simultaneously to the same victim. Types of trafficking can include forced sex work, pornography, strip dancing, criminal enterprise and bonded labor in domestic servitude or migrant work. Outside of street sex work, sex trafficking is most likely to be occurring in venues such as strip clubs, massage parlors, or other fictitious business fronts. A major difference with sex trafficking of minors is that, unlike adults, force, coercion, or fraud does not need to be present for prosecution (6). As there are a number of different avenues for and types of human trafficking, recognition can be challenging.
Risk Factors
The profile of the human trafficking victim is not easy to define. Victims of human trafficking come from varied backgrounds that may or may not be what is expected or stereotypical. Victims may come from any race, socioeconomic status, color, religion, age, gender, sexual orientation or gender identity. The main commonality is that there is a layer of deception whereby the human trafficker is targeting a vulnerability in the victim. As stated by the Department of Justice, trafficking victims are deceived with “. . . false promises of love, a good job, or a stable life and are lured into situations where they are made to work in deplorable conditions with little or no pay” (5). There are some trends noted that do make certain populations more at risk, but keep in mind that this does not encompass all potential victims and vigilance should be taken to avoid assumptions.
The risk factors for human trafficking are just as varied and dependent upon the type of trafficking and method by which the abuser is able to hold the victim indentured or captive. This figurative prison may be physically, emotionally, or monetarily induced. The Center for Disease Control and Prevention (CDC) lists the following characteristics and factors:
- Many victims are women and girls, though men and boys are also impacted.
- Victims include all races, ethnicities, sexual orientations, gender identifies, citizens, non-citizens, and income levels.
- Victims are trapped and controlled through assault, threat, false promises, perceived sense of protection, isolation, shaming, and debt.
Several higher risk populations have been identified through the data gathered from the Polaris Project. It was found that children who were or had been within the foster care system or runaway homeless youth were more likely to encounter sexual victimization. Other factors include substance abuse, recent relocation or migration, unstable housing situations, and underlying mental health disorders (7).
As a population that is often overlooked, shamed, or lacks resources, members of the lesbian, gay, bisexual, transgender, queer, plus (LGBTQ+) community are more vulnerable to being subject to human trafficking. Up to 40% of homeless youth are part of the LGBTQ+ community and may not seek assistance for fear of being shunned (8).
Illegal and sponsored immigration remains at a higher risk of trafficking and exploitation. The NHRTC reports a significant number of calls that reference foreign nationals (2). Individuals wishing to become American citizens are lured with the promise of freedom in exchange for large fees that are made impossible to be worked off. Although there are laws in place to prevent this, this type of servant bondage is forced upon the victims who are in a new country and often lack resources or are unable to seek assistance due to cultural, language, and accessibility barriers. Further, cases have been reported where the employer or trafficker withhold visas or identification barriers in order promote compliance and essentially are holding the victim hostage (9).
Mandatory Reporting
Mandatory reporting of human trafficking by health care professionals is incorporated into the law in a growing number of locations in the United States. Health care professionals are already mandated reporters through previous existing laws that require reporting of child abuse, domestic violence, as well as knife and gunshot wounds (11)
The following states the criminal and civil liability of failing to follow the law as a mandatory reporter in some states:
In a civil action, the mandated reporter may be held liable for all damages that any person suffers due to the mandated reporters’ failure to file a report. In a criminal action, the mandated reporter may be found guilty of a misdemeanor punishable by imprisonment for up to 93 days and a fine of $500.
Reporting of suspected adult human trafficking is not as clear in regard to mandatory reporting. However, vulnerable adults suspected of being abused, exploited, or victimized fall under the same guidelines and are reported to the Centralized Intake (CI) at the Department of Health and Human Services in the same manner as above.
Recruitment Techniques
A major tactic of the perpetrators of these crimes is to prey on vulnerable individuals with a lack of resources. Thus, a primary ploy used is a layer of deception whereby the human trafficker is targeting the needs or wants of the victim.
Traffickers are often individuals that the victim has come to trust. This may be a girlfriend or boyfriend, intimate partner, spouse, or other family member. Victims are also commonly sold to outside parties.
In cases of sexual trafficking, typically young women and men are groomed and given preferential treatment, gifts, and drugs until they become reliant upon the “John”. In other cases, individuals are tempted with the promise of a better life, or in the case of immigration, the sponsorship for a visa (9).
Federal Laws
Today, there are 39 states that have committed to the crusade of establishing a statute banning human trafficking.
A specific U.S. Federal law addressing trafficking crimes was first enacted with the Trafficking Victims Protection Act of 2000. The bill has since been revised several times; however, the fundamental of it is to provide guidance and authorization for their “three-pronged approach that includes prevention, protection, and prosecution” and covers both sex and labor trafficking (12).
Preventing Sex Trafficking and Strengthening Families Act of 2014 and The Justice for Victims of Trafficking Act of 2015 are both aimed at providing victims increased protection for exploitation and increased resources specifically aimed at prevention and support for child and youth sex trafficking crimes (12).
The Customs and Facilitations and Trade Enforcement Reauthorization Act of 2009 is aimed towards prohibiting the importation of goods made by victims of human trafficking (12).
Self Quiz
Ask yourself...
- Do your state's requirements align with what you have read in this course concerning federal law mandates?
- What is your mandated responsibility regarding human trafficking?
Self Quiz
Ask yourself...
- What is your mandated responsibility regarding human trafficking?
Recognizing Signs of Human Trafficking
According to the Department of Health and Human Services, close to 90% of human trafficking victims visit a health care facility at least once while in servitude and are not identified as such by health care providers (14). This is due to a lack of education, lack of consistent use of identification and screening tools, and time constraints within the current health care system. As a mandatory reporter and healthcare team member, it is imperative to use best practice in recognizing the signs and symptoms as well as the tools that are available.
Signs and Symptoms
Human trafficking victims may present to a healthcare setting with primary or underlying signs that may be related to physical or mental abuse. These signs and symptoms may be related to the reason that they are seeking treatment or may be identified by the healthcare provider during a thorough assessment. The following physical and psychological sequelae may be noted during an assessment as potential evidence of victimization (all derived from 9, 15):
Physical
- Unexplained or implausible injuries
- Bruising
- Wounds and Cuts
- Missing or broken teeth
- Closed head injuries
- Blunt force trauma
Neurological
- Headaches
- Migraines
- Memory loss or difficulty concentrating
- Vertigo
- Insomnia
- Brain trauma
Gastrointestinal
- Diarrhea
- Constipation
Dietary
- Malnutrition
- Anorexia
- Severe weight loss
Cardiovascular and Respiratory
- Tachyarrhythmias
- Hypertension
- Respiratory distress
Reproductive System
- Sexually transmitted disease
- Vaginal and/or anal fissures
- Previous Abortions
Psychological
- Depression
- Suicidal Ideation
- Anxiety
- Self-harm including cutting or branding
- Drug and alcohol abuse
- PTSD symptoms
- Regression
- Anger
- Dissociative and depersonalization tendencies
Red Flags and Indicators
There are several characteristics that should be kept in mind as red flags during the interview and assessment that may indicate potential trafficking. These include, but are not limited to (all derived from 9, 15, 16):
- Tattoos that indicate ownership, a number, or tracking system or are out of character/obscene
- Inappropriate clothing for climate
- Workplace violence or abuse
- Unsanitary living conditions
- Multiple families or people sharing a living space that is too small
- Shares living space with employer
- Is not in control of financial assets
- Refusal to speak alone with health professionals
- Accompanied by individual that refuses to allow patient to speak for themselves or be alone
- Sex work under age 18
- Answers are scripted
- Answers are implausible or contraindicated
- Appears younger or older than stated age
Self Quiz
Ask yourself...
- Which of these red flags and indicators of human trafficking stand out to you?
Interview Tools and Techniques
Check with your facilities protocol for specific guidance on assessment and examination protocols for suspected abuse victims. There are also many scripted interviewing tools available online that assist with asking targeted questions. First and foremost, it is important to establish the patient’s safety and to gain trust.
Gaining trust can be difficult and conducting assessments and interviews should be completed in a non-threatening environment with an unbiased and non-judgmental tone. Creating a space that is quiet and will not be interrupted is important. This will ensure that the potential victim feels safe communicating and is not concerned that they will be overheard. Present your demeanor in a non-threatening manner, at eye level, and focus on being attentive with observant listening. Maintain respectful eye contact to convey interest and reflective listening. If taking notes during the interview is required, explain to the patient what will be documented and what it will be utilized for (17).
The National Human Trafficking Resource Center (NHTRC) offers a plethora of resources and scripted questions. The following are general questions on assessing if the individual is being forced into a situation and can be applied to any of the specific types of human trafficking (all from 17):
“Did someone control, supervise or monitor your work/your actions?”
“Was your communication ever restricted or monitored?”
“Were you able to access medical care?”
“Were you ever allowed to leave the place that you were living/working? Under what conditions?”
“Was your movement outside of your residence/workplace ever monitored or controlled?”
“What did you think would have happened if you left the situation? Was there ever a time when you wanted to leave, but felt that you couldn’t? What do you think would have happened if you left without telling anyone?”
“Did you feel that it was your only option to stay in the situation?”
“Did anyone ever force you to do something physically or sexually that you didn’t feel comfortable doing?”
“Were you ever physically abused (shoved, slapped, hit, kicked, scratched, punched, burned, etc.) by anyone?”
“Were you ever sexually abused (sexual assault/unwanted touching, rape, sexual exploitation, etc.) by anyone?”
“Did anyone ever introduce you to drugs, medications as a method of control?”
While screening tools provide a base for asking difficult questions, the NHTRC advises “Before screening, users should also be prepared to draw upon the expertise of local legal and medical staff and to refer identified trafficking victims to appropriate housing, health, and social services in their area . . . the tool is a complement to, not a substitute for, specialized training in human trafficking, good professional practice and victim-centered service” (17).
The NHTRC also provides a 24-hour national hotline that is able to guide health professionals through completing assessments and determining the next best steps to intervene or offer the victim assistance. This is a very beneficial resource; however, it must be understood that calling NHTRC does not fulfill the mandatory reporting requirement for certain states and the Centralized Intake (CI) at the Department of Health and Human Services is the only means of legally fulfilling the reporting obligation.
Self Quiz
Ask yourself...
- Think about an actual real-life scenario in which you are interviewing a victim of human trafficking. How would you begin the interview? What tools would you use?
Interventions and Collaboration
When presented with a suspected human trafficking victim, it is likely that the individual will not be alone. Maintaining safety and support for the patient may require separation from the suspected trafficker. While this may not be possible, an attempt should be made to bring the patient to a room or examination area unaccompanied.
Be conscious of any cultural preferences that may affect the patient. If there are language barriers preventing meaningful communication, enlist the assistance of a professional interpreter. This is especially vital in cases where the accompanying visitor or family is attempting to interpret for the patient and may be filtering the victim’s responses.
For patients that seek healthcare related to sexual abuse, a SANE assessment and rape kit should be obtained per facility protocol. With permission, patients should be tested for sexually transmitted infections including HIV, gonorrhea, UTIs, syphilis, and pubic lice, as well as a pregnancy test for females. Forced and coerced abortions are frequent among minor females in the sex industry (18).
Thorough documentation of the patient’s reported reason for visit, physical and neurological assessment including any trauma, bruising, wounds, affect, and pertinent statements should be noted in the patient’s electronic medical record.
Educate yourself on local resources and be able to provide assistance with finding access to healthcare, mental health, and rehabilitative resources that are available in the community. Victims may not want to take pamphlets with them that may be found, so providing locations or addresses of shelters or clinics with operating times may be a safer option.
Collaborate with the healthcare team, law enforcement, and social work for suspected child or vulnerable adult trafficking.
Mandatory reporting of suspected cases of child abuse or trafficking is not encumbered by HIPAA disclosure when reporting to authorities; however, when reporting suspected adult trafficking, disclosure and permission must be granted unless there is an imminent threat to the safety of the patient, or the patient has been identified as a vulnerable population. Thoroughly assess if the individual meets criteria as a vulnerable adult and proceed accordingly. If the adult does not meet criteria, permission must be gained to report.
If a competent adult does disclose that they are a trafficking victim, determine if the patient is in immediate, life-threatening danger. If so, follow facility protocol and encourage and support the patient in reporting to a law enforcement agency. If there is no immediate danger, supportive care and assistance should be provided. The patient should be informed of the options available for social services, reporting, and resources. Creation of a safety plan is highly recommended (15).
Self Quiz
Ask yourself...
- What opportunities for collaboration are there in your community?
Prevention
Prevention of human trafficking requires public education, awareness, and knowing how to properly respond when faced with suspicions. The Blue Campaign is a strategy from the Department of Homeland Security to bring national awareness to the issue and provide specialized training to law enforcement and federal employees. Blue Campaign pamphlets and other materials are available at their website, www.dhs.gov/blue-campaign, for distribution.
The Center for Disease Control takes the stance that sex trafficking is preventable via community awareness and acknowledging exploitation when it does occur. They state “Strategies based on the best available evidence exist to prevent related forms of violence, and they may also reduce sex trafficking. States and communities can implement and evaluate efforts that:
- Encourage health behaviors in relationships
- Foster safe homes and neighborhoods
- Identify and address vulnerabilities during health care visits
- Reduce demand for commercial sex
- End business profits from trafficking-related transactions” (6).
One of the largest barriers to prevention in the healthcare system is the inability to recognize signs and symptoms. As cited above, a significant number of human trafficking victims have filtered in and out of healthcare systems without being recognized. These are missed opportunities to connect, provide resources, and offer further assistance. The NHTRC provides many resources for training within healthcare facilities and standardized forms and interviewing questions that may be tailored to individual situations and facility needs.
Resources
National Human Trafficking Resource Center
Phone: 1-888-373-7888
SMS Text: 233733 (Befree) – Text “HELP” OR “INFO”
Online chat: https://humantraffickinghotline.org/chat
This network provides healthcare facilities and individuals with information and connections to over 3,200 referral contacts that will assist human trafficking victims. These contacts include low or no-cost legal services, law enforcement agencies, social services, and anti-trafficking organizations. Communication is enhanced as dialect is available in English, Spanish, and 200 other languages.
HEAL (Health, Education, Advocacy, Linkage) Trafficking
Website: www.Healtrafficking.org
The HEAL Trafficking Direct Service Committee works to improve the clinical care for trafficked persons by providing opportunities for service providers to connect, access support, share information and promising practices, identify best practices, and expand the referral network.
National Center for Missing & Exploited Children
Address:
333 John Carlyle Suite 125
Alexandria, VA 22314-3175
Phone: 1-800-THE LOST (1-800-843-5678) 24-Hour Call Center
Website: http://www.missingkids.org/theissues/trafficking
Provides specialized technical assistance, analysis, and recovery services on cases involving child sex trafficking.
Pain Management in Nursing
Pain is a subjective, complicated symptom that afflicts every human at some point in their lives. Pain management in nursing within healthcare settings is a challenge and must take into consideration patient-centered preferences, treatment goals, as well as guidelines and laws from governing bodies. For many years, opioids were the first line of defense against acute and chronic pain conditions. With the opioid crisis, this mindset has been required to change.
The Epidemiology of Pain
Pain is a subjective, complicated symptom that afflicts every human at some point in their lives. Managing pain within healthcare settings is a challenge and must take into consideration patient-centered preferences, treatment goals, as well as guidelines and laws from governing bodies. For many years, opioids were the first line of defense against acute and chronic pain conditions. With the opioid crisis, this mindset has been required to change.
Due to an overabundance of prescribing opioids, the opioid related death toll has continued to rise. Not only has this fatal epidemic resulted in untimely deaths for many, it is estimated that "For every 1 prescription opioid death, there are 20 specialty substance abuse treatment admissions, 45 emergency department visits for nonmedical use and adverse events, 156 people with substance use disorder and dependence, and 533 people using the drugs nonmedically overall" (1).
This public health crisis has resulted in the conviction of pharmaceutical companies that were behind the political stronghold monopoly on pain management in America. As a result, the Federal government has collaborated with The Institute of Medicine (IOM) and the Centers for Disease Control (CDC), among many other experts in the field, to develop a plan that protects the American public from unintended opioid use and promotes a multi-disciplined, multi-modal approach to combating pain in America.
Self Quiz
Ask yourself...
- What is your current understanding of the different types of pain people can experience, as well as common treatment methods?
- What actions can be taken to determine a patients pain level during an assessment?
Statistics to Consider on Pain Management in Nursing
Pain is a widespread public health concern that reaches every corner within America. In a 2011 report titled, Relieving Pain in America: A Blueprint for Transforming, Care, Education, and Research, the IOM revealed that pain affects nearly 100 million Americans and nationally costs upwards of 635 billion U.S. dollars each year (2). Of these numbers, over 25 million American adults report that they suffer from pain daily, while 23.4 million state a significant amount of pain (3).
Researchers gathered data from 8,781 American adult participants regarding individual perceptions of their overall health, underlying illnesses, and pain experiences within the previous three months. This study ranked pain on a scale of categories from one through four, with one being the least amount of pain, and four being the highest level of pain.
From this data, it is estimated that almost 40 million individuals ranked themselves as living with pain at a category three or four. Individuals in these categories were also found more likely to have an accompanying disability, access healthcare on a more frequent basis, and have an overall worse quality of health and life (4).
Self Quiz
Ask yourself...
- Do these statistics surprise you? Why or why not?
- How many individuals ranked themselves as living with high category pain in 2011?
What is Pain and Why Does it Occur?
Merriam-Webster defines pain as "a localized or generalized unpleasant bodily sensation or complex of sensations that causes mild to severe physical discomfort and emotional distress and typically results from bodily disorder (such as injury or disease) (5)".
Pain is the body's defense to achieve a response against further damage from a perceived threatening stimulus. The brain perceives pain via specific pathways. Four stages of pain transmission occur: transduction, transmission, perception and modulation (6).
Receptors within afferent fibers are activated when a potential threatening stimulus occurs. This initiates three stages of pain perception. Initially, pain sensitivity is triggered. From there, signals follow a network of peripheral neural pathways towards the spinal cord. Within the spinal cord is the dorsal horn, which contains neurons that translate and relay information about the painful or irritating peripheral stimulus to the thalamus and cortex in order to elicit a protective response (6,7).
Pain can be further distinguished within two frameworks, chronic and acute, and by pain related conditions, such as inflammatory responses, nociceptive, and physiological dysfunctions.
Self Quiz
Ask yourself...
- How would you have previously defined pain?
- How does this prior understanding compare to the definition outlined in this course?
Identifying Types of Pain for Pain Management in Nursing
Pain is classified by three distinct types: nociceptive, inflammatory, and neuropathic. The following are general descriptions of the types of pain; however, it must be noted that these pains can overlay each other and be occurring simultaneously.
Nociceptive Pain
Nociceptive pain is due to nerve impairment or injury and is the most common type of pain that occurs. It is sometimes noted as being central pain that is caused by repeated or harmful stimuli. The nociceptors activated in this type of pain are spread throughout the body within internal organs, bones, joints, and the integumentary system (6).
Nociceptive pain is generally described as radicular, somatic, or visceral depending on the nerve involvement. Examples of nociceptive pain include the sensation from touching a hot object, a broken arm, or a paper cut at the initial time of injury. It may also describe pain caused by cancer, arthritic changes, and ischemic pain that does not originate from nerve injury.
Inflammatory Pain
Inflammatory pain is part of the cascade of sequelae that makes up the immunological defense to damage caused by heat, toxins, trauma, foreign substances, or infection. Neutrophils, along with prostaglandins, histamine, and other chemical mediators flood the location of injured tissues as a part of the bodies normal, inflammatory response. Classic signs include erythema, edema, and heat at the site of injury (6). Inflammatory pain can be seen in cases of an ankle sprain, cellulitis, and allergic reactions.
Neuropathic Pain
Neuropathic pain is also often associated with a phenomenon called allodynia. Allodynia is the sensation of pain from an activity or event that is typically not associated with causing pain. Rather than being the result of a physiological event, neuropathic pain is pathologic in nature.
According to Yam, Loh, Tan, Adam, Manan, and Basir (2018), "This condition can be described as "pathologic" pain, because neuropathic pain actually serves no purpose in terms of defense system for our body, and the pain could be in the form of continuous sensation or episodic incidents" (6). It is thought to be caused by disorders affecting the peripheral or central nervous system and is linked to diseases that cause nerve damage such as trauma, toxins, diabetes, as well as certain viral infections, such as herpes zoster.
Self Quiz
Ask yourself...
- Think of a patient you have encountered in your practice who experienced chronic pain.
- How would you classify this patient’s pain?
- What are the key differences between each type of pain?
- What are some examples of each type of pain?
Chronic Pain vs. Acute Pain
Acute pain is that which is short-term and self-limiting. Generally, the timeframe of acute pain is based on the expected healing process of the injurious event and may be up to six months.
Chronic pain lasts beyond the expected period of healing or is recurrent. Acute pain can usually be attributed by a defined contributing factor or event, such as appendicitis or a broken bone. Chronic pain can be related to a myriad of causes or the etiology may be unknown (6).
In clinical settings, pain lasting more than three months is typically used to define the transition from acute to chronic. As such, chronic pain must be treated and managed differently than acute pain.
Risk Factors
Several risk factors have been identified that make it more likely for an individual to experience chronic pain. In general, age influences the prevalence of chronic pain by population, with those age 18 to 39 having an increased prevalence of chronic pain. This may be due to other age groups under-reporting.
Those over 80 were found to report acute pain more often but were less likely to acknowledge chronic pain when asked. As well, cognitive decline, dementia and other age-related diseases must be considered as factors when collecting data. Chronic pain after surgery is reported at a higher rate amongst adolescents (7).
Chronic pain is more likely to be experienced and reported by females over males. However, studies have shown that women experience pain differently than males at a lower threshold. Women have been found to be more likely to seek treatment for pain (7,8).
Certain co-morbidities have been identified that are linked to an increase of chronic pain.
Almost 90% of patients reporting chronic pain have significant co-morbidities. Co-morbidities with the highest link to chronic pain are cardiovascular and respiratory diseases and depression. The link between chronic pain also affects mortality rates. In those reporting severe chronic pain, the 10-year survival rate decreases significantly. At ten years, those reporting severe chronic pain are twice as likely to have died from ischemic heart disease or respiratory disease than those with little to no pain (7).
Depression and anxiety are reported at a rate four times higher in individuals with chronic pain than those living without pain (7). Specific conditions that have a higher rate of being linked to mental health disorders include (all from 8):
- Arthritis
- Fibromyalgia
- Back/Neck pain
- Chronic migraines
- Menstrual-related pain
Other factors that have been found to influence the prevalence of reported chronic pain include (7,8):
- Poverty
- Self-identify as minority
- Obesity
- Manual labor occupations
- Unemployed
- Smoker
- Alcohol use
- Lack of physical activity
- Poor nutrition
- Low levels of Vitamin D
- Post-surgical and medical interventions
- Sleep Disorders
Self Quiz
Ask yourself...
- What co-morbidities have the highest link to chronic pain?
Physical and Psychological Elements of Pain
Pain elicits a response from the sympathetic nervous system (SNS) leading to signs and symptoms affecting all systems of the body. The following are some of the physical effects that pain may cause within each individual system.
With the sensation of pain, the cardiovascular system anticipates an event that is threatening. The SNS produces a rush of adrenaline and cortisol that results in tachycardia, hypertension, and increased oxygen demand.
The respiratory response includes elevated breathing that is shallow. The cortisol levels have an effect on the endocrine system, resulting in a surge of glucose by triggering a release of glucagon from the liver that will keep up with the demands needed for the fight or flight response.
In contrast, with chronic pain, continued elevated cortisol levels may lead chronic hyperglycemia. The gastrointestinal system slows gastric motility which may lead to nausea, vomiting, and constipation.
Chronic pain may lead to an increase in gastrointestinal discomfort, including irritable bowel syndrome. The urinary tract reacts to stress with oversensitivity leading to an increased urgency to urinate, and possibly incontinence (7).
Physical indications of pain from the musculoskeletal system are displayed as pilo-erection, tremors, and muscle tension and rigidity. The nervous system reconfigures with the processing of pain and attempts to adapt to the additional stresses. Repeated episodes of acute pain can increase the risk of an individual developing chronic pain.
Cumulatively, the stresses and changes that occur on these systems have a negative effect on the immune system. The immune system is unable to keep up with the demands and becomes desensitized to repeated inflammation culminating in a lowered immune response. The lowered immune response then poses an increased risk of infection for the individual (5).
Psychological Responses
Pain can cause a wide array of psychological symptoms that are subjective and may be difficult to quantify. These include anxiety and fear, poor concentration, and inhibitory or promotory effects on pain (7). When pain is experienced, the activation of certain parts of the brain induce a heightened awareness and fear as a defense mechanism. Part of this process also provides a certain level of natural analgesia.
With long-term pain this results in continued activation of this system, leading to increased risk for depression, anxiety, and abnormal sleep patterns (7). As stated by Swift (2018), "A high threat level induces strong emotions such as fear or intense anxiety, leading to a state of high arousal, awareness and/or vigilance, which in turn reduces sensitivity to pain. A low or moderate threat level causes a less intense response, such as low-level anxiety or depression, which induces a low-to-moderate state of arousal in which pain is more easily felt" (7).
Self Quiz
Ask yourself...
- What are some long term effects of chronic pain on the body?
- Have you ever personally experienced pain or treated a patient with chronic pain that led to anxiety, depression, or a sleeping disorder? How was this managed?
Pain Management in Nursing
As guidelines have changed due to the opioid crisis, new evidence published by the CDC suggests that opioid dependency can occur in as little as a ten-day course of treatment.
In addition, the American Pain Society and the American Society of Anesthesiologists have released guidelines that stress a multi-modal approach to pain management in the operative and recovery setting. Of the recommendations, the following were released as having high-quality evidence and strongly recommended (as cited in 8):
". . . that clinicians offer multimodal analgesia, or the use of a variety of analgesic medications and techniques combined with nonpharmacological interventions, for the treatment of postoperative pain in children and adults"
". . . that clinicians provide adults and children with acetaminophen and/or non-steroidal anti-inflammatory drugs (NSAIDs) as part of multimodal analgesia for management of postoperative pain in patients without contraindications"
". . . that clinicians offer neuraxial analgesia for major thoracic and abdominal procedures, particularly in patients at risk for cardiac complications, pulmonary complications, or prolonged ileus"
". . . that clinicians consider surgical site-specific peripheral regional anesthetic techniques in adults and children for procedures with evidence indicating efficacy".
The shift has moved from starting patients on opioids after surgeries or other pain inducing procedures, to treating pain using the multi-modal approach which stresses using alternatives to opioids as the first line of defense. The CDC further recommends and advises (8):
"Nonopioid medications are not generally associated with development of substance use disorder. The number of fatal overdoses associated with nonopioid medications is a fraction of those associated with opioid medications. Nonopioid medications are also associated with certain risks, particularly in older patients, pregnant patients, and patients.
With certain comorbidities such as cardiovascular, renal, gastrointestinal, and liver disease. Nonpharmacological treatments can reduce pain and improve function in patients with chronic pain. These treatments can also encourage active patient participation in the care plan, address the effects of pain in the patient's life, and can result in sustained improvement in pain and function with minimal risks. If opioids are used, they should be combined with nonopioid medication and nonpharmacological treatments, as appropriate."
Pharmacological Pain Treatments (Adapted From )
Opioids may be used for moderate to severe acute or chronic lower back pain, osteoarthritis, and neuropathic pain. Studies showing long-term efficacy are extremely limited. Opioids are suggested only after other non-opioid and non-pharmacological therapies have failed to provide relief. This class should be used with caution as it may induce sedation, respiratory depression, nausea and vomiting, and constipation.
Short Acting
- Codeine
- Hydrocodone/acetaminophen or ibuprofen
- Oxycodone/acetaminophen or ibuprofen
- Hydromorphone
- Morphine
- tramadol
Long Acting
- Fentanyl
- Hydrocodone
- Methadone
- Morphine
- Oxycodone
- Oxymorphone
- Tapentadol
Anticonvulsants may be used for fibromyalgia, diabetic and other neuropathies, and neuralgias. Use with caution as significant drug-drug reactions have occurred. Dosing should be adjusted for renal impairment. May cause sedation, dizziness, dry mouth, weight gain, and edema.
- Gabapentin
- Pregabalin
- Carbamazepine
- Valproic acid
Antidepressants are commonly prescribed for fibromyalgia, low back pain with radiculopathy, migraines, neuropathies and neuralgias, and chronic musculoskeletal pain. Patient must be monitored for mood changes and is at an increased risk for suicide.
Other side effects may include sedation, urinary retention, dry mouth, weight gain, and blurry vision. Cardiac patients must be monitored for arrythmias and blood pressure changes.
Tricyclic Antidepressants
- Amitriptyline
- Desipramine
- Nortriptyline
Serotonin-Norepinephrine Reuptake Inhibitors
- Duloxetine
- Milnacipran
- Venlafaxine
Muscle Relaxers are effective for acute lower back pain and fibromyalgia. May cause sedation and dizziness. Caution must be used when operating a car or machinery.
- Carisoprodol
- Cyclobenzaprine
- Metaxalone
- Methocarbamol
- Tizanidine
Topical agents are particularly helpful for osteoarthritic and rheumatoid arthritic pain as well as neuropathies. May be used for relief of sprains, strains, and back pain.
- Capsaicin
- Diclofenac Topical Gel
- Lidocaine 5% patches
- Menthol/Salicylate
Non-Steroidal Anti-Inflammatory Drugs may be used to treat backache, joint pain and inflammation, headache, arthritic pain, muscle aches, strains, and menstrual cramps.
Caution should be used in patients with liver or kidney disease and alcohol misuse. May cause gastrointestinal discomfort or bleeding. Use with caution if patient is on anticoagulation therapy.
- Ibuprofen
- Diclofenac
- Indomethacin
- Meloxicam
- Naproxen
- Celecoxib
- Aspirin
Acetaminophen remains one of the most commonly prescribed pain relievers for headache, backache, muscle ache, and joint pain. Caution must be used with liver disease and alcohol misuse. Dosage must not exceed 3,000-4,000 mg/day.
Interventional Treatments include epidural or intraarticular glucocorticoid injections and arthrocentesis. The CDC recommends these for short-term treatment of inflammatory diseases such as rheumatoid arthritis, osteoarthritis, rotator cuff disease and other radiculopathies.
Self Quiz
Ask yourself...
- What are some examples of long-acting opioids?
- What are some examples of short-acting opioids?
- Why is it so important to monitor for mood changes with antidepressants?
- What are the challenges of opioid use and abuse when it comes to pain management in nursing?
Non-Pharmacological Treatment
The CDC provides many strategies for healthcare providers to manage the challenges of patient pain control in a manner that lessens the need for opioid use and provides alternative options. Primarily, a patient-centered approach to treatment is now the gold standard and should include patient engagement.
Suggestions and strategies to incorporate patient cooperation and engagement with their pain management plan include (all from 9):
- Use reflective listening by maintaining eye contact, empathizing, and confirming understanding
- Set agreed upon, reasonable and achievable goals
- Discuss treatment options using a multi-modal treatment plan
As part of a multimodal therapy in treating pain, the CDC highly recommends incorporating exercise along with other psychologically based approaches into care. The following are non-medicinal forms of pain management:
- Physical and occupational therapy includes exercise such as swimming, yoga, walking, free weights, and other strength training. This can improve strength and posture, which may provide relieve from lower back, hip, and osteoarthritic pain, improve fibromyalgia symptoms, and has been shown effective in preventing migraines (9).
- Cognitive behavior therapy (CBT) is a psychosocial training technique that addresses modifiable situation factors and cognitive processes that may affect the experience of pain. CBT aims to provide coping techniques, relaxation methods, and may include self-help instruction, professional counseling, or support group attendance (9).
- Heat Therapy
- Cryotherapy
- Massage
- Ultrasound
- Transcutaneous Electric Nerve Stimulation (TENS) units
- Acupuncture
- Hypnosis
- Stress Management
- Chiropractic Manipulation
- Herbal Preparations
- Aromatherapy
Self Quiz
Ask yourself...
- Can you think of a patient experience where you used cognitive behavior therapy principles to help better manage their pain? Do you think it was effective? Why or why not?
Federal Laws on Opioid Prescribing and Use
In 2016, the CDC reported that over 40 Americans were dying each day due to prescription opioid overdoses. The opioid crisis has been attributed to the over prescribing of opioids for pain and non-pain conditions with a lack of oversight leading to a 400% increase in opioid prescribing and sales since 1999 (10).
In response, the federal government implemented an initiative to combat the issue with improved education, guidelines, and treatment management. In October of 2018, the Substance Use Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities Act, a 660-page bill was signed into law.
This comprehensive, bi-partisan legislation aimed to provide funding and expand access in order to increase treatment availability through Medicaid and Medicare, expand alternative non-opioid pain management treatment, set guidelines for improved patient education, and identify best practices (11).
Prescription-drug monitoring program and the use of electronic prescribing for Schedule II and III medications is supported by the Federal government and allows individual states to have primary control over authorization and enforcement.
Drug Classification and Schedules In the United States
As determined by 21 USC 802(21)(A) and 21 USC 813, state and federal agencies monitor certain drugs based on their risk of addiction, dependance, and abuse characteristics.
These controlled substances are categorized based on a system of Schedules I through V. There are three criteria that determines the drugs category: acceptable medical use, potential for abuse, and the predictive value of dependance if it is abused (12, 13). The schedules are as follows:
Schedule I drugs are considered to have no appropriate medical use and have an extremely high potential for abuse. Examples of Schedule I drugs include:
- LSD
- Heroin
- Bath Salts
- Quaaludes
Schedule II drugs have a high potential for abuse and may lead to psychological or physical dependance. Examples of Schedule II drugs include:
- Fentanyl
- Demerol
- OxyContin
- Morphine
- Codeine
- Marijuana
Schedule III drugs have a high potential for abuse and may lead to psychological or physical dependence. Examples of Schedule III drugs include:
- Acetaminophen with Codeine
- Vicodin
- Suboxone
- Ketamine
- Anabolic Steroids
Schedule IV drugs have a low to moderate potential for psychological or physical dependence but have a lower risk for abuse. Examples of Schedule IV drugs include:
- Ativan
- Xanax
- Valium
- Soma
- Klonopin
Schedule V drugs are a low potential for physical or psychological dependence or abuse. Examples of Schedule V drugs include:
- Gabapentin
- Robitussin
- Ezogabine
- Phenergan with Codeine
CDC Guidelines and Recommendations on Prescribing and Use
The CDC continues to promote guidelines initiated in 2016 to support the U.S. government's initiative to curb the increasingly troubling deaths related to opioid overdose. These guidelines were aimed at assisting primary healthcare providers in effectively managing and treating patient's pain while addressing health and safety concerns. In relation to opioid use, the guidelines revolved around three main principles (all from 8):
- Nonopioid therapy is preferred for chronic pain outside of active cancer, palliative, and end-of-life care.
- When opioids are used, the lowest possible effective dosage should be prescribed to reduce risks of opioid use disorder and overdose.
- Providers should always exercise caution when prescribing opioids and monitor all patients closely.
Drug Diversion Within the Healthcare System
According to the Drug Enforcement Administration, the most commonly abused drugs are among five classes and are frequently used in the treatment of pain. These include opioids, depressants, stimulants, hallucinogenic, and anabolic steroids. Of these, the opioid fentanyl is the number one drug that is found to be involved in drug diversion cases (14).
When used outside of medical purposes, fentanyl has an extremely high rate of fatality. Far from being just a public problem, the diversion of drugs is a significant problem for healthcare organizations and abusers can be found at all levels, from the C-suite to frontline staff.
There are several signs of drug diversion, including poor appearance, failing job performance, uncharacteristic behaviors for the individual, and accessing medication that is not required for their job (17).
The Joint Commission offers these guidelines for monitoring to identify potential trends and patterns that may indicate the occurrence of drug diversion in the clinical setting (all from 14):
- Schedule II - V substances are removed:
-
- Without provider orders
- Under patients not assigned to the nurse
- Under patients that have been discharged or transferred
- Excessively by one individual
- Substitute drug is removed and administered while controlled substance is diverted'.
- Verbal order for controlled substances is created but not verified by prescriber
- Prescription pads are diverted and used to forge prescriptions for controlled substances
- Provider self-prescribes controlled substances
- Patient alters written prescription
- Unadministered medication that is documented as given to patient
- Wastes are not completed according to policy and procedures
- Multiple discrepancies or overrides are noted
- Patient's report unrelieved pain, despite increasing documented pain medication administration
- Assistance is frequently offered to administer medications for other nursing staff
- Expired controlled substances go missing or are diverted from medication dispensing systems
Individual policy and procedure should be followed when drug diversion is recognized in a clinical setting with consideration to the safety of the patients and offender both addressed. The drug diversion should be reported to an immediate supervisor or manager. Nursing management should contact Quality Control and initiate a thorough root-cause analysis.
Risks of drug diversion include transmission of blood borne pathogens, patient safety compromised due to impaired healthcare provider, uncontrolled patient pain, and potential for healthcare provider overdose.
The Joint Commission advocates for a "see something, say something" approach to combatting healthcare provider drug diversion. A plan to prevent drug diversion within the health care organizations should include three approaches: prevention, detection, and response.
Additionally, they state "Detection of drug diversion is challenging, and even the best efforts have not yet achieved complete eradication of diversion. Patient and workplace safety require effective reliable safeguards to maintain the integrity of safe medication practices to protect against diversion. Diversion prevention requires continuous prioritization and active management to guard against complacency" (15).
Self Quiz
Ask yourself...
- What can you do as a healthcare provider to prevent drug diversion?
- Have you seen specific examples of drug diversion in your workplace?
- What can you learn from that situation?
Risks of Opioid Use and Misuse
Opioids target mu receptors in the brain and spinal cord. Through inhibition of GABA, dopamine is released. Opioid's increased risk for addiction is due to the increase of circulating dopamine which is associated with increased pleasure responses.
Opioid use has been clinically linked to an increase in addiction as well as substance use disorder. Substance use disorder has been defined by the American Psychiatric Association (APA) as ". . . a problematic pattern of use of an intoxicating substance, leading to clinically significant impairment or distress" (16).
Per the APA, this is calculated by at least two of the following characteristics (all from 16):
- The substance is often taken in larger amounts or over a longer period than it was intended
- There is persistent desire or unsuccessful effort to cut down or control use of the substance
- A great deal of time is spent in activities necessary to obtain the substance, use the substance, or recover from its effects
- Craving or a strong desire or urge to use the substance
- Recurrent use of the substance, resulting in a failure to fulfill key role obligations at work, school, or home
- Continued use of the substance despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of its use
- Important social, occupational, or recreation activities are given up or reduced because of use of the substance
- Recurrent use of the substance in situations in which it is physically hazardous
- Use of the substance is continued despite having knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance
- Tolerance: a need for markedly increased amounts of the substance to achieve intoxication or desired effect OR a markedly diminished effect with continued use of the same amount of the substance
- Withdrawal: characteristic withdrawal syndrome for that substance OR the substance (or a closely related substance) is taken to relieve or avoid withdrawal symptoms
A comparison study was performed based on information garnered in a 2016-2017 study group that focused on the use and misuse of opioids among individuals medicating with opioids inappropriately. This group was split into four categories and compared medical prescription opioid users with prescriptions with the following: misusers without prescriptions, misusers of own prescriptions, and misusers with both types of misuse (14).
Individual misusers without a prescription were typically younger, male, and unmarried versus misusers with prescriptions, whether using medically or misusing. It was found that misusers also had an alcohol disorder, used marijuana, and misused benzos and stimulants. As well, noted was that misusers were more likely to be nicotine dependent and to use cocaine and/or heroin (14).
Prescription users were more likely to concurrently use prescribed benzodiazepines and stimulants. Depression among all misusers was higher compared with the medical users. The misuser also more commonly had received treatment from an inpatient mental health treatment center as well as had been prescribed a medication for a mental health condition. Overall, this group was not more likely to have a physical health condition (14).
Perceived Barriers to Pain Management in Nursing
As another consequence of the opioid crisis, a stigma has been cast upon individuals with chronic pain whether they are taking opioids or not. Healthcare professionals should be cautioned against projecting biases onto sufferers of pain as seeking pain medications for misuse reasons.
As previously detailed, many patients experiencing pain have co-morbidities and are at a higher risk of having mental health issues in addition to pain.
Barriers to non-opioid and non-pharmacological pain control may include insufficient medication regimen ordered to address patient's pain, inadequate training, nursing workload, and a lack of collaborative approach by the healthcare team (17).
Barriers to the use of non-pharmacological pain relief methods have been cited as (all from 17):
- Inadequate training of personnel in how to examine pain and non-pharmacological control methods
- Patients' lack of cooperation in the use of non-pharmacological methods to relieve pain
- Insufficient knowledge about non-pharmaceutical pain relief methods
- Time-consuming methods of nonpharmaceutical pain relief
- Nurse's reluctance to use non-pharmaceutical pain relief methods
- Failure to use non-pharmacological methods by the physician
The study found that with improved education, communication, and collaboration, improved pain management can be achieved by patients.
Self Quiz
Ask yourself...
- What are some steps that you as a healthcare provider can take in preventing the stigma with chronic pain patients as it relates to opioid use?
- How can you administer pain relievers using best practice?
Nursing Considerations and Interventions
Nursing care plans focused on pain management may be categorized by acute or chronic pain; however, the management and interventions are similar for each. The outcomes should be specific to the patient presentation, disease process, and preferences (18).
Pain Assessment and Screening Tools
Screening tools are one of the easiest and most effective ways to evaluate for pain. Some of the most commonly used in clinical care include (6, 18, 19):
- Wong-Baker FACES Scale - may be used for children over the age of 3 and adults
- FLACC and CRIES - used for infants
- COMFORT Scale - May be used in children and cognitively impaired or sedated adults
- Visual Analog Scale
- Numerical Rating Scale
Pain should be also assessed by the patient reported characteristics using pain standardization scales such the McGill Pain Questionnaire. Some of the verbiage used to describe pain include (6):
- Aching
- Burning
- Shooting
- Stabbing
- Throbbing
- Tender
In addition to screening tools, the nursing assessment should include visualization of signs of pain that can include guarding or protecting certain areas of the body, facial changes such as grimacing or furrowing of brows, and other manifestations of pain such as restlessness, moaning, or crying (5).
Self Quiz
Ask yourself...
- Which of the pain scale tools have you used in your professional practice?
- Do you think they were effective in helping you determine your patients’ level of pain?
- Do you think one is more effective than another?
Conclusion - Nursing Interventions Related to Pain Management in Nursing (All from 18)
- Provide therapeutic communication and patient-centered care, taking into consideration patient preference.
- Assess and document patient baseline of vital signs, complete head-to-toe assessment, and review medications.
- Assess and document patient pain through use of a pain scale, and responses to interventions.
- Establish an agreed upon pain level that is acceptable to the patient, providing education that no pain at all is not a reasonable goal.
- Administer pain medications per physician orders.
- Regularly assess for sedation in patients who are receiving pain medication.
- Administer naloxone for patients presenting with clinical signs of over-sedation with opioid use.
- Provide education on and integrate alternative pain t per patient preference and provider orders.
As nurses, being able to have a firm concept of the different types of pain, the contributing factors that lead to pain and the various modes of treatment will allow you to provide better care for your patients, while simultaneously allowing you to relate to them on a more specific level and formulate a more individualized plan of care.
Drains: Everything you Need to Know
Drains are often placed in patients to allow for drainage of a site. The most common indications for drains is to evacuate abscesses, infections, and/or excess fluids . Nurses caring for patients with drains are often intimidated and overwhelmed. In this CE course you will learn about drain management and how care for patients with drains.
Introduction
Picture this: you walk into your hospital unit, fresh off a good night’s sleep. You find your patient assignment and head over to get report. Then the outgoing nurse says something that makes your heart skip a beat. “This patient has an abscess drain. You need to flush it every X hours, record the output every X hours, call the doctor if __ happens…” Before long, your head is spinning, and then you realize you’ve been spelling ‘abscess’ incorrectly for who knows how long! You think to yourself “I really need to know more about the nursing care of drains!”
Drains can be intimidating, especially with little to no prior experience in drain management. They often come with a specific set of instructions that can be somewhat confusing. What’s worse, a patient may suffer a serious delay in recovery if something goes wrong. Nobody wants to be the one to make that call to the doctor about a malfunctioning drain. Fortunately, like anything else, managing drains becomes much easier with experience and a little education.
Types of Drains
A patient may require drain placement for various reasons. Often, they are placed at the end of a surgery or percutaneously to help eliminate any fluid that may accumulate within the wound. A common type of surgical drain is the Jackson-Pratt ® . Certain organs may require a drain to assist with the removal of their contents, such as foley catheters or nasogastric tubes. Drains may also be placed to help remove fluid or air from body cavities. A chest tube is a good example of this type of drain. Finally, if a patient develops an abscess, a drain is often required to help remove the infected fluid more quickly.
Drains serve a very important purpose (other than driving the patient and his/her nurses crazy). The accumulation of fluid in the wrong place can have a detrimental effect on the patient’s health and healing (1). Excess fluid in the surgical site can cause significant pain as well as injury to surrounding tissues and organs (1). It can also increase the chance of infection (1).
Medical drains can be divided into multiple categories.
Drains are often described as being active or passive. Passive drainage allows for gravity to help remove excess fluid, without the use of pressure (2). An example of passive drainage would be placing a foley catheter to gravity or using a penrose drain. A penrose drain is a relatively flat, ribbon-like tube that creates a passage from a wound to the open air, which allows any excess fluid to simply flow outward (2). The area surrounding the opening is often lightly covered with gauze to collect fluid as it drains and must be changed when saturated (2).
The following image is an example of a penrose drain (3).

Active drains use actual pressure, typically negative pressure, to help remove excess fluid from the body.
An example of an active drainage system would be a Jackson-Pratt (JP) ® drain or hemovac ®. With both types of drains, the pressure is created by compressing the collection container, which creates a low pressure vacuum that pulls the fluid out of the body (2). The following images are examples of hemovac (12) and JP ® drains (3).
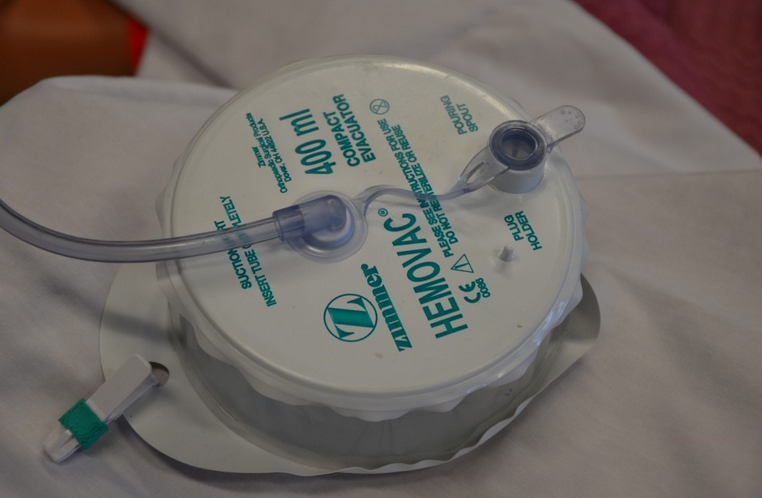
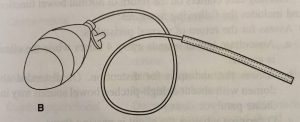
Self Quiz
Ask yourself...
- Why is it important to know the different types of drains?
Open vs. Closed Drains
Drains can also be described as open or closed. An open system simply means that it is open to air. An example of an open system would be a penrose drain, as described above. A closed drain, on the other hand, is not open to the environment. Rather, the draining fluid is contained within the system, and the collection bulb or bag is simply emptied from time to time, as needed. A JP ® drain is an example of a closed drain.
Surgical vs. Percutaneous Drains
While not a technical classification, it is interesting to note how the drain is placed. Surgical drains are usually positioned in the operating room or, more rarely, at the bedside by the physician. The JP ® is an example of a surgical drain.
Drains may also be placed percutaneously:
Percutaneous: (adjective) effected or performed through the skin (4)
Percutaneous drains are placed without surgical intervention. Rather, Interventional Radiologists use imaging, such as CT, ultrasound, or fluoroscopy to guide a needle into a fluid collection (5). This technique is generally less invasive (6). Before surgical or percutaneous insertion of a drain, the patients coagulation status and hemostasis risk must be evaluated (13).
Self Quiz
Ask yourself...
- What are the advantages and of open versus closed drainage systems?
Infections 101: A Brief History of Drains
Before the advent of antibiotics, the development of an abscess or postoperative infection was often a death sentence (7). Thanks to advances in modern medicine, suffering patients now stand a chance. In certain situations, infections can be treated simply with a course of antibiotics. However, if there is any concern for the development of sepsis, further intervention is needed (6).
Until the 1970s, the most effective (and only) way to treat infection and abscess was surgical intervention (7). Surgeons would attempt to remove the infected material while striving for “directness, simplicity, and above all, avoidance of unnecessary contamination of uninvolved areas” (7). Unfortunately for these patients, this meant that a second surgery was required to heal them from complications of their first surgery. Even with the addition of antibiotics, these situations were associated with significant morbidity and mortality (6).
Luckily, rapid advances in technology allowed for the development of a less invasive solution. The advent of fluoroscopy, ultrasound, and especially CT provided physicians with a tool to see inside the body without having to cut someone open. The first studies involving the use of medical imaging for percutaneous drain placement were published in the late 1970s (7). Over the next several years, multiple studies reported success rates ranging from 60-80% using these new techniques (8).
Doctors are now able to drain up to 3 separate abscess/infection sites percutaneously (8). Recent studies report technical success of up to 90% with percutaneous drain placement, and it can offer immediate improvement in sepsis, with return to hemodynamic stability within 1-2 days (9). CT is considered the imaging modality of choice because of its ability to fully visualize the infection and surrounding structures as well as provide a pathway from the skin to the destination (9).
Self Quiz
Ask yourself...
- How has the increased use of medical drains altered the medical care and approach to managing abscesses?
Patient Considerations for Percutaneous Drain Placement
Not every infection or fluid collection requires percutaneous drain placement or even surgery. Thus, it is important for physicians to work together to determine the appropriate treatment for each patient individually. When a patient is found to have an abscess, multiple doctors may get involved, usually either a surgeon or interventional radiologist (sometimes both) and a clinical pharmacist if an infection is suspected or confirmed.
It is essential that providers choose patients carefully, as ineffective or incomplete drainage of the infection can lead to significant morbidity and mortality (8). For example, percutaneous drainage is sometimes avoided in patients with chest infections, such as empyema, abscess, and pleural effusion because of the risk of pneumothorax (9). Additionally, pyogenic and fungal abscesses in the lung parenchyma often resolve with more conservative management, namely through supportive care and antibiotics (9). Pancreatic abscesses remain at high risk of treatment failure with percutaneous drain placement, thus surgery is usually still the intervention of choice (9).
Conversely, there are many types of abscesses that respond well to percutaneous drainage. Liver abscesses have a very low risk of complications with this type of drain placement, around 1-4% (9). It is also very effective in managing infections related to visceral perforation, which may result from Crohn’s disease, prior operations, diverticulitis, and appendicitis (9). Deep pelvic abscesses respond well to percutaneous drainage, although these can be more challenging and require careful planning because of the presence of nearby organs (9).
Percutaneous drainage is often considered for patients who are too ill for surgery, in the hopes that it may improve sepsis and promote increased strength/rest (8). It is also recommended for patients who have a good response to antibiotics and low risk of mortality.
Self Quiz
Ask yourself...
- Deciding who may benefit from a drain and who needs conservative therapy is difficult and nuanced.
- How would you consult with on this subject?
- Should medical therapy be initiated while awaiting intervention?
Image-Guided Drainage: How Does it Work?
When first contemplating percutaneous drainage, doctors must first decide which modality to use: fluoroscopy, ultrasound, or CT. As mentioned previously, CT is most often used to guide drain placement because of its superior visualization.
The interventional radiologist will typically review any available imaging beforehand to plan the most appropriate route for drain placement. Care must be made to avoid major vessels and other important structures (6). To minimize the risk of complications, physicians are advised to use the safest, most direct route and attempt placement in the most dependent part of the fluid collection to encourage effective drainage (6).
Once the patient is properly positioned on the table, the physician will use the CT, ultrasound, or X-ray to guide the placement of a special needle, taking frequent pictures to monitor its progression from the skin through soft tissue and into the infection (6). Once the needle is in place, a wire is passed through the needle into the fluid collection and then the needle is removed, leaving only the wire in place.
Next, a drainage catheter is threaded across the wire to its final resting place. The tip of the catheter rests within the fluid collection. The drainage catheter contains holes to help fluid pass out of the body. Once the tube is in place, the wire is removed. A drainage bag is attached. Throughout the procedure, pictures are taken to ensure correct placement. Patients are often given moderate sedation to make them more comfortable, but not in every case.
Drain Management
Care for the patient with a drain can seem intimidating, but it doesn’t have to be. Often, the physician will write orders to guide nursing staff while caring for these patients. Drain management may also differ depending on what type of drain the patient has. If there are no orders it is reasonable to contact the physician who placed the drain for clarification.
Surgical Drains
Two of the more common types of surgical drains are the hemovac ® or JP ® drain. As mentioned previously, both of these drains are active, closed systems, meaning they use negative pressure to help remove excess fluid from a surgical wound, all of which is stored within the collection device.
When managing JP ® or hemovac ® drains, it is important to note the color of the drainage fluid. The fluid is typically bloody or purulent at first, but should gradually lighten to a light pink, clear, or yellow color (10). Indications for removal may vary, but in general, these drains remain in place until the daily output decreases to less than 30 ml (10).
Follow any written instructions provided by the ordering physician. Nurses will also be responsible for emptying the drain, observing the site and documenting findings. The drain should be emptied no later than when it becomes half full, as it will lose suction and become ineffective (2). Observe the insertion site for drainage and signs of infection. Be sure to keep the skin clean. These drains may also be sutured in place. The drains should be further secured with medical adhesive or pinned to the patient's gown with a safety pin to secure the drains before mobilizing and to avoid accidental removal.
Percutaneous Drains
Percutaneous drains usually look a little bit different. The interventional radiologist uses a special type of drainage tube that is also sometimes called a ‘pigtail’. These tubes do not always have to be sutured in place, for they may contain a string that, when pulled, curls the distal end of the tube, making it a bit harder to pull out. They are then usually adhered to the skin with a dressing.
Again, it is important to note the color of the drain output. Keep in mind that percutaneous drains are often used for abscess or infection, meaning fluid will be purulent and/or bloody. Check for any specific written instructions for drain management. Monitor the drain site regularly for signs of infection or drainage. Empty the drainage bag as directed or as needed and document findings. These drains may also use a collection bag that applies suction through negative pressure.
Percutaneous abscess drains are more likely to require flushing because the purulent drainage can be thick and pose a risk for occluding the drain. They may be equipped with a three-way stopcock to allow for easy flushing.
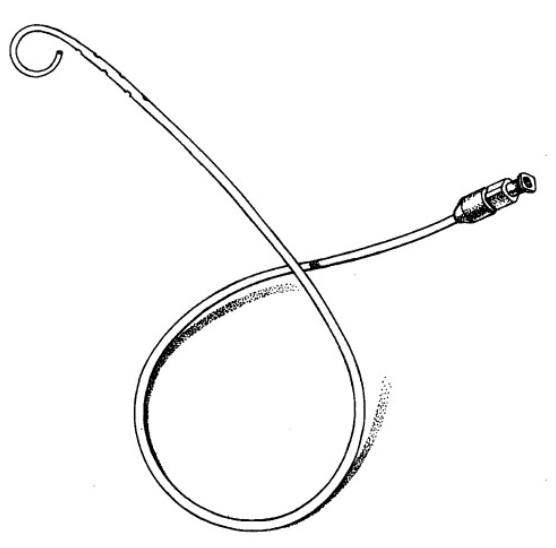
(French pigtail catheter [Cook Inc., Bloomington, IN; C-PCS-830-LOCK]).
Self Quiz
Ask yourself...
- Image guidance has revolutionized drain placement. Don't you think?
- What are the advantages of surgical drains and what is their role currently?
How to Flush a Drain Using a Three-way Stopcock
The first step is to review any written orders and become familiar with policies regarding drain flushing. You may be required to have a provider order in order to flush a drain. Then gather some supplies: gloves, an alcohol pad, “dead end” cap or clave, clean pad/towel, and saline flush syringes. Prepare by applying gloves and laying out a clean towel or pad underneath to create a workspace and catch any drainage. Flushing a drain is usually painless, but advise patients that they may feel a little discomfort.
Take a look at the figure below (11). It is an example of a three-way stopcock. It has three different ports and an “off switch” that swivels. Whichever direction the off switch is pointing closes that port so fluid cannot flow. In the example provided, the switch is closed to the patient, meaning that fluid cannot pass into the bag.
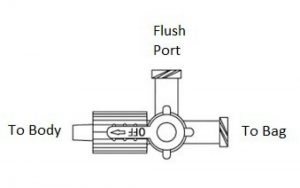
Step 1. Find the Flush Port
To flush the drain, find the flush port located on the stopcock. It should be pretty easy to spot, as it is usually the only port that is free (since one end of the stopcock is connected to the actual drain tube, the other to the drain bag). The flush port should be capped with either a “dead end” cap or a clave. If there is a dead end cap, it will have to be removed, since saline cannot be flushed through. If a clave is present, the saline syringe can be screwed in directly.
Step 2. Prepare the Flush Port
Next, turn the off switch so it is pointing toward the flush port, if it isn’t already. This will close the flush port or “turn it off” so that drainage cannot leak out. If a dead end cap is present, remove it. Wipe the flush port with an alcohol pad and attach a new, sterile clave, if available. Claves make future flushing much easier because the flush syringe can be attached directly. If a clave is already present, wipe it thoroughly with an alcohol pad.
Step 3. Prepare the Saline
Attach a saline syringe to the flush port. 5-8 ml is usually plenty. If the ordering physician wrote specific instructions on how much saline to infuse, follow the directions closely. The off switch will have to be turned before flushing is possible. At this point, the switch is facing the flush port, which prevents fluid from exiting or entering. The attached saline simply will not flush, no matter how hard the plunger is pushed.
Step 4. Flush the Drain
Saline can be flushed either into the drain or into the bag, depending on which way the off switch is turned. To flush the drain itself, a nurse would have to direct the saline toward the patient. This means the off switch needs to be turned toward the bag. The bag is now “off” and won’t get any flow, allowing saline to travel through the flush port and up the drain into the patient. Once the saline is flushed, turn the off switch back to the flush port. This will reopen flow into the bag. The saline that was just infused should now travel freely through the drainage tube and into the bag. Observing this allows the nurse to know that the tube is draining correctly.
Sometimes the contents of the abscess can be thick or contain particles that can clog the tube leading to the bag. Thus, the drain bag may also need to be flushed. Simply follow the same steps listed above, only, instead of turning the off switch to the bag, it should be turned to the patient. This will prevent flow from entering the drainage tube, leaving a pathway from the flush port into the drain bag. The nurse should be able to see the saline traveling into the bag. Once the bag is flushed, return the off switch to face the flush port. This allows for an open pathway from the drain into the bag.
Step 5. Assess the Drain
After flushing, it is important to note any patient discomfort, as well as document how much saline was flushed.
Before leaving the bedside, and always when assessing a patient’s drain, ensure that the off switch on the stopcock is turned toward the flush port. This will allow drainage to flow seamlessly from the patient into the bag.
Note that not all drains are meant to be flushed, especially those that do not contain a flush port and/or three-way stopcock. Never flush a drain without a provider’s order. Do not attempt to flush a drain if you suspect it has been pulled away from its original position.
Properties of a Well-Functioning Drain
Since humans lack x-ray vision, the inner workings of a drain can seem a little mysterious. What is going on in there? How can a nurse know if it is doing what it is supposed to do? Repeat imaging (CT, ultrasound, etc.) is the best way to visualize how infections and abscesses change over time. However, it is costly and unnecessary to expose patients to extra radiation as a matter of curiosity.
To get some idea of how a drain is functioning, one has to look at the drain itself. Even though drains may look different, they function in similar ways, thus these considerations can be applied to both surgical and percutaneous drains.
Output
The hallmark of a well-functioning drain is output. The purpose of a drain is to get fluid out of the body. Therefore, if the collection bag/bulb is capturing drainage fluid, this is a good indication that it is working correctly. Remember that the fluid is often bloody at first, but should lighten over time. The drainage from an abscess may also be bloody at first before appearing purulent.
Skin Site Clean/Dry
The skin at the site of a drain should be kept clean and dry (2). Minimal amounts of fluid may leak around the tube, causing crusting on the skin or a small amount of visible drainage. This can be gently wiped away with clean gauze soaked with normal saline or warm, soapy water (10). Apply a fresh clean gauze at the site to protect the skin from breakdown (10). If a large amount of drainage is leaking from the skin and around the tube, this is not normal and should be addressed.
Stopcock in the Proper Position
Ensuring that the three-way stopcock (if present) is in the proper position is essential for proper function. The off switch should be pointing to the flush port at all times, unless the nurse is preparing to flush the drain. Turning the off switch to the flush port prevents fluid from draining outside the system and creates an open pathway from the drain into the drain bag.
Active Suction
All active drains should be monitored closely to ensure that the bulb or accordion is adequately compressed (2). Constant negative pressure must be maintained in order for the drain to work. To compress a JP, use the "side-in method" where the nurse compresses the JP bulb at its largest diameter (in the middle) with fingers and thumb to compress the bulb (14). The drain should be emptied when it is approximately 25 percent full to maintain the pressure within the bulb (14).
These drains may require frequent assessment and emptying, especially at first. Examples of active drains include JP®, hemovac®, and most percutaneous drains.
Is this Normal? Drain Troubleshooting
Unfortunately, drains can develop complications. It is essential to know what to look for so that potential problems can be identified early. As mentioned previously, a delay in reporting or discovering a drain malfunction may cause delays in patient healing. Luckily, the problems are fairly easy to spot if you know what to look for.
Bleeding
Some bleeding is normal. The act of placing a drain may cause bleeding from nearby small vessels (9). This is usually self-limiting, which is why the nurse may note bleeding in the early hours after placement. The drainage should gradually lighten. Prolonged bleeding or the development of new bleeding warrants a prompt call to the physician.
Leaking
A leaky drain can be a messy business. If the source of the leak is not immediately known, the nurse should evaluate the drain. Assess the tubing for cracks or holes. Ensure all connections are tight. Sometimes the drainage bag/bulb may be punctured. If so, it is often easily replaced.
Leaking may also occur because the drain is occluded or kinked (2). Assess the tubing carefully for signs of obstruction. Flushing the drain can help dislodge occlusions. Again, never flush a drain without orders from the physician.
A drain may also leak at the skin. Minimal amounts of leakage can be expected because the drain creates a track for small amounts of fluid to escape. Moderate to severe leakage can cause skin breakdown and is not normal. It suggests that the drain is malfunctioning in some way, often due to an occlusion or displacement of the drain. Fluid travels the path of least resistance. If it can’t pass easily through the tube, it will find another way out. Notify the physician, who may order follow up imaging, like a CT scan. If a percutaneous drain is leaking, the patient may have to be sent down to interventional radiology for assessment and possible replacement.
No Output
Drain output may cease for two reasons: there is no more fluid or the fluid can’t get out. It is easy to assume the former. Yet, when faced with a drain without drainage, It is important to use critical thinking and common sense. Drainage usually tapers off, meaning it will drain a little less over time. An abrupt cessation of fluid could indicate a problem. Assess the drain for kinks or obstructions. If the drain is occluded, fluid may begin to leak around the tube at the skin. Carefully document drain output as dictated by the physician or facility protocol. Any time there is a concern, the physician should be notified.
Infection
Infection may occur with both surgical and percutaneous drains. It usually forms one of two ways: during initial drain placement or as a result of continued catheter presence (9). Infection may form during initial placement if the needle punctures a non-target area (such as the colon) or from prolonged dilation, which is why the procedure should be completed in a timely manner (9). Infections may also form at the skin if a drain is present for a long time (9).
The nurse should assess the drain site frequently. Signs of skin infection include redness, increased pain, swelling, fever, and purulent drainage (10). Additionally, sepsis is always a concern for the patient with an abscess (9). A patient with sepsis will sicken very quickly, with rapid increase in fever, chills, and rigors (9). Vital sign monitoring is essential. If the nurse suspects a new infection of any kind or deterioration, notify the physician immediately.
Displacement
Living with a drain takes some getting used to. It can be easy for patients to forget it’s there. Sometimes the tubing can become tangled up in the bed sheets or left behind when a patient stands up. Although drains come equipped with reinforcements, such as a suture or dressing to help keep the tubing in place, it is possible to pull the drain at least partially or sometimes completely out of the body.
If a drain is pulled out entirely, the nurse should cover the site with some gauze to catch any drainage. When drains are placed, they form a pathway from the abscess or infection to the skin. The tube’s job is to provide a conduit for the fluid to escape. If the tube is removed abruptly, that pathway still exists temporarily, so fluid will continue to leak out of the body in the absence of the tube. Do not attempt to put the tube back in, as it is no longer sterile. Notify the physician.
If the drain is only partially removed, reinforce the dressing as best as possible to maintain its current position and call the physician. Again, do not attempt to push the tubing back inside the patient. The physician may order imaging to assess the drain’s location (2). Removal and/or replacement may be necessary.
Self Quiz
Ask yourself...
- Managing drains can be intimidating at first. Would you agree?
- How would you troubleshoot the common issues listed here?
Summary
This course is designed to help readers become more familiar with drains. They come with all sorts of indications: to facilitate healing after surgery or infection, to assist with draining contents from affected organs, or remove fluids that have accumulated in body cavities.
Drains are classified based on their function: open or closed, passive or active. Familiarity with the different types of drains gives the nurse a basic understanding of how they work- which is important because they can look very different, depending on the manufacturer.
In the old days, surgery and antibiotics were the only way to treat intra-abdominal infections. Significant advances in technology have allowed interventional radiologists to specialize in using medical imaging (CT, ultrasound, X-ray, and MRI) to place drains without making an incision. However, patient selection is still very important, and physicians must know which patients are good candidates for percutaneous drain placement and which are better off heading to the OR.
This course is also designed to provide a basic understanding of drain management and troubleshooting. It is important for nursing staff to understand how a drain is supposed to behave when it is functioning normally so that potential problems are easier to spot. When in doubt, consult the physician. Always be aware of any written orders or policies that dictate drain management, as practices may vary from place to place.
As with anything else, the best way to become more comfortable with drains is to be around them!
Administration of Blood Products
Administration of blood products is one of the many responsibilities we have as nurses. Almost 21 million blood components are transfused each year in the U.S (1), each with the potential for harm. Unfortunately, many preventable transfusion errors occur each year. Staying up to date on blood administration is the best way for nurses to avoid potentially deadly consequences of transfusion errors.
Introduction
Administration of blood products is one of our many responsibilities as nurses. Around 14 million blood components are transfused annually in the U.S. [6], each with potential harm. Unfortunately, many preventable transfusion errors occur each year. Staying current on procedures for administering blood products is the best way for nurses to avoid the potentially deadly consequences of transfusion errors.
You float to an oncology unit and are assigned three patients who receive blood. Does this scenario increase your heart rate? Some nurses administer blood and blood products daily, while others are less familiar and may need a reminder of the administration basics.
The goal of the course is to teach safe administration of blood products.
Administering blood can be daunting, but if you remember the basics, you and your patient will be safe. Before diving in, let's look at some exciting blood facts by the Red Cross [1,2]
- Approximately 29,000 units of red blood cells are needed daily in the U.S.
- Around 16 million blood components are transfused each year in the U.S.
- The average red blood cell transfusion is about three units.
- The blood type O is the most often requested by hospitals.
- A victim from a single car may require as many as 100 units of blood.
- An estimated 6.8 million people in the U.S. donate blood annually.
- About 45% of Americans. have Group O (positive or negative) blood; 57% of Hispanics and 51% of African Americans also have Type O
- 7% of the U.S. population has type O negative blood, which is always in high demand since it can be given to patients of all blood types.
- Type AB plasma can be transfused to patients of all blood types, and only 4% of people in the U.S. have A.B. blood.
Self Quiz
Ask yourself...
- How has the availability of blood transfusions affected your life or the life of one of your family members?
- Are you comfortable with a patient's choice to not receive blood products, even if it means they will die?
- What are your personal beliefs regarding blood transfusions and why?
Pre-Infusion / Pre-Administration of Blood Products
There are many steps before the infusion starts; the most important is to verify, verify, verify [3,4,6,7].
Verify the physician's order.
No order? No blood – it's that simple.
Standard blood orders include whole blood, red blood cells, and leukocyte-reduced RBC.
Whole blood is the simplest, most common type of blood donation. It's also the most flexible because it can be transfused in its original form or separated into specific components such as red cells, plasma, and platelets. Whole blood treats patients needing blood components, such as those with significant blood loss from trauma or surgery.
Red blood cells (RBCs) are prepared from whole blood by removing the plasma. RBCs treat anemia without increasing the patient's blood volume too much. Patients who benefit most from transfusion of red blood cells include those with kidney failure or gastrointestinal bleeding and trauma.
Leukocyte-reduced RBCs are prepared by removing leukocytes (white blood cells) by filtration after donation before the RBCs are stored. This is done because, over time, the leukocytes can deteriorate, triggering adverse reactions in the patient who receives them.
Verify the patient has signed a blood consent.
The only time you can transfuse blood without written consent is for emergency treatment. In this rare situation, the physician may verbally order to infuse blood emergently without a concrete written order.
Pre-Infusion Checklist
- Check if premedication is required.
- Premedication such as acetaminophen and or diphenhydramine may be required for patients who have acquired antibodies from multiple transfusions in the past. An example of this is sickle cell patients.
- Check for special requirements (such as CMV negative).
- Special requirements may be needed for patients who have acquired antibodies from prior reactions or illnesses like cancer.
- Verify if the patient has had a history of blood transfusion reactions.
- If they have had a history, find out their reaction and ensure this information is shared with the ordering physician.
- Discuss the order with the patient and explain the process to the patient.
- Even though they signed a consent, this is a new part of their treatment plan and must be included. Include teaching about signs and symptoms of transfusion reaction. More discussion on this topic is below.
- Verify the patient has an active type and cross.
- Blood can only be distributed with this information if in an emergent situation. Type and cross screens are typically valid for three days.
- Review the patient's morning laboratory reports.
- Pivotal labs to monitor include potassium, as it may rise with transfusion; BUN/Cr to ensure kidney function; hemoglobin and hematocrit for the severity of the anemia; PT/PTT/INR/Platelets to evaluate the coagulation status of your patient.
Self Quiz
Ask yourself...
- Think about the last time you administered blood to a patient- now reflect on your teaching regarding the infusion. Will it be different next time? Why?
- What would be different in infusing blood in a patient with a past hemolytic reaction?
- Your patient has a serum potassium of 5.7 mEq/L, has renal failure, and needs three units of PRBC's. How will you approach this discussion with the healthcare provider?
Assess Your Patient
Why is your patient getting blood? It would help if you documented this to understand the clinical picture. As the nurse, this is important so you can develop a baseline to know if anything changes with your patient during the infusion process.
It is essential to understand how to perform the following critical assessments in addition to baseline vitals.
- Neurological Assessment – Alert and oriented to what? Is the patient at their baseline neurological status? Any changes?
- Pulmonary Assessment – What are their breath sounds like? Any crackles? How are their respirations at rest? What did the morning chest x-ray look like? Are they on oxygen? How much? What is the pulse oximetry reading? Any weight gain overnight? Pedal edema?
Any patient at risk for fluid volume overload needs to be identified (such as patients with heart failure or renal disease). If you are concerned that your patient is experiencing fluid volume overload while administering blood products, discuss this with the healthcare provider who ordered it. Options may include slow administration of the blood product or premedicating with furosemide [7,8].
Baseline Vital Signs (1, 3, 5)
- Temperature – The patient should be afebrile. If they are febrile, do not order or administer blood unless the physician orders to transfuse despite their knowledge of fever.
- Heart Rate – Rate, rhythm, and pulse quality should be documented.
- Respirations – Rate and rhythm should be documented.
- Blood Pressure – Baseline blood pressure should be documented for the patient. Is it "normal" for the patient? What is the trend?
Determine IV Access
The IV gauge for routine blood infusions should be 20 gauge or larger in adults, and for rapid transfusions, nurses may use a 16 to 18-gauge IV [7]. The larger the IV, the quicker blood can be administered. The IV line should be used for blood only. Nothing else can be transfused with blood [7].
Blood tubing must always be primed with 0.9% normal saline. Normal Saline is the only fluid in which blood products should be infused. Blood tubing, called Y tubing, has a 170-260 micron filter. Blood tubing must be replaced with every unit of blood or every 4 hours, whichever comes first and depends on hospital protocols [7]. Depending on your institution, blood warmers and pumps may be optional or mandatory.
Self Quiz
Ask yourself...
- If your patient is showing signs of fluid overload prior to an infusion but still needs the blood, what options would you discuss with the ordering provider?
- Your patient has only one line and is receiving multiple antibiotics, what will you do?
- If your patient is neurologically compromised at baseline, how will this alter the way you will observe for signs of a blood transfusion reaction?
Infusion / Administration of Blood Products
Once the blood is removed from the blood bank, it should be infused within 20 to 30 minutes, or returned blood must be infused within 4 hours [7,8]
Now that you have the blood in hand and a patient with a grand IV, grab your nearest Registered Nurse (RN), Medical Doctor (MD), or appropriate second verifier (Determined by your institution) and verify, verify, verify ([5,6,7].
Typical Blood Verification Checks include:
- Patient name
- Medical record number
- Date of birth
- Patient blood type
- Donor blood type
- Unit/pool/lot number
- Product type
- Special preparations (i.e.; Leuko-reduced)
- Rh factor
- Expiration date and time of blood
- Visually inspect bag for damage
- Visually inspect blood for color difference or clots
*Remember: This is a suggestion of the main points of a blood infusion checklist. Your institutional policy determines the definitive checklist by which you should administer blood. *
Before administration, two licensed personnel should verify the correct blood product and match it with the patient. This should be done at the patient's bedside using the identifying band on the patient for verification as well as the patient themselves (if possible) [5,6,7].
The Importance of Two-Step Verification
Did you know that the most frequent error leading to transfusion of ABO-incompatible Blood occurs during patient identification at the bedside? As a result, although the blood is labeled appropriately, it is transfused to someone other than the correct recipient [4].
The problem with transfusion errors and accurate patient identification led to one of the 2024 National Patient Safety Goals to "use at least two patient identifiers when providing care, treatment, and services” [10]. To prevent this from occurring, The Joint Commission requires (before initiating a blood or blood component transfusion):
- Match the blood or blood component to the order of the physician or provider.
- Match the patient to the blood product.
- Use a two-person verification process [9].
When using a two-person verification process, one individual conducting the identification verification is the qualified transfusionist who will administer the blood or blood component to the patient [9]. When using a two-person verification process, the second individual conducting the identification verification is qualified to participate, as determined by the hospital [9].
Now that you have verified blood and are infusing the product, it is not the time to go to lunch. Stay with the patient during the first 15 minutes of transfusion to monitor for any immediate reaction and start the infusion slowly. Vital signs should be repeated 15 minutes after the beginning of the transfusion, during the procedure per facility policy, at the conclusion, and one hour after the transfusion [7,8].
The rate of the actual infusion should be based on a) if a rate was ordered, b) ensuring the infusion is complete within the allotted 2-4 hour time frame, and c) nursing judgment related to the patient's hemodynamic and pulmonary status [7].
Self Quiz
Ask yourself...
- The most frequent error leading to transfusion of ABO incompatible blood occurs during patient identification/verification at the bedside . How does that make you feel as a nurse? Why?
- Have you ever observed nurses checking blood away from the bedside? What was your response and why?
- How would you feel if you of your family member were given the wrong blood because of a verification error at the bedside?
Reassessment of Vital Signs
- Neurological Assessment – Changes in baseline neurological assessment, including lethargy, confusion, or any decrease in Glasgow Coma Scale, may indicate a transfusion reaction.
- Pulmonary Assessment – Any changes from baseline? Oxygen requirement changes? Saturation changes? Signs of increased pulmonary secretions or pulmonary edema? These are signs of fluid overload and may indicate a transfusion reaction.
- Temperature – An increase is often a sign of a transfusion reaction.
- Heart Rate – Tachycardia or arrhythmias may signify a transfusion reaction.
- Respiration – An increase in respiration may be a sign of a transfusion reaction or fluid volume overload.
- Blood Pressure – An increase in B.P. may be a sign of fluid overload, but a significant decrease is a sign of a transfusion reaction.
- IV Access – Still patent? Infusing without difficulty? At the prescribed rate? [8].
Blood Transfusion Reactions
Why must you stay in the room and reassess everything in 15 minutes?
If the patient is going to experience an acute blood transfusion reaction, it usually takes place within the first few minutes of infusion.
There are many signs and symptoms of blood transfusion reactions for hemolytic and non-hemolytic reactions [6,7,8].
Hemolytic Reactions |
Non-Hemolytic Reactions |
| Pain | Pain |
| Anxiety | Anxiety |
| Hematuria | Hematuria |
| Fever | Fever |
| Headache | Headache |
| Pruritus | Pruritus |
| Rash or Hives | Rash or Hives |
| Nausea | Nausea |
| Respiratory Difficulties | Respiratory Difficutlies |
| Bleeding | |
| Hypotension | |
| Oliguria |
If a reaction is suspected, the transfusion should be immediately stopped, blood products and tubing removed, and the intravenous line kept open with normal Saline. The provider should be notified immediately, and the patient should be monitored. The remaining blood products and tubing should be taken to the laboratory [5,7,8]. Refer to facility policy and procedure for documentation and other requirements. Labs must be drawn as part of a suspected transfusion reaction workup.
If all goes well, continue to monitor the patient according to your facility’s protocol during the remainder of the infusion. If there are no changes after 15 minutes in assessments or vital signs, vital signs should be repeated at least every hour and at the conclusion [7,8]. Again, refer to your facility policy, as this can vary.
Post-Infusion / Post-Administration of Blood Products
Once the administration of blood products is complete, obtain a set of vital signs. Compare to baseline and 15-minute vital signs. If you haven’t already done so, complete documentation:
- Start/Stop time
- Pre, 15-minute, and post-infusion vital signs
- Blood volume infused
- 0.9% Normal Saline volume infused
- Signs & Symptoms of transfusion reaction, if any
- Reason for transfusion
- Answer "yes" or "no" to suspected transfusion reaction
- Document in the notes how the patient tolerated the infusion
- Properly dispose of blood and blood tubing in a red waste container
- Flush the IV access with Saline
Now, wait – you aren't done yet! Remember that non-acute blood transfusion reactions can occur hours after the infusion, so continue to monitor and assess your patient closely. Remember to document the one-hour post-infusion vital signs and complete any post-infusion labs that may have been ordered [7,8].
Knowledge about any skill improves your confidence and results in safe patient care. Hopefully, this has improved your understanding of the administration of blood products and increased your confidence in performing this procedure!
Self Quiz
Ask yourself...
- Have you ever witnessed a blood transfusion reaction? Do you think you could identify a reaction?
- In an unstable patient, would it be more difficult to "catch" a transfusion reaction? Why or why not??
- What is your institutions response to the 2020 National Patient Safety Goals of eliminating transfusion errors related to patient misidentification? How would you find this information?
Institutional Policies on the Administration of Blood Products
All organizations have different policies, it is important to review your institutional policy regarding the administration of blood products. It is your responsibility to learn your institution’s policies regarding the administration of blood products and to follow them appropriately. Documentation is per institutional policy and should include the reason for the infusion as well. Every institution has a procedure for releasing blood products. Follow the institutional policy to obtain the blood to have it to infuse in a timely manner.
A Nurse’s Guide: How to Deal with Difficult Patients
Introduction
Being in the business of caring for people when they are at their worst means we often come face-to-face with patients amid emotional outbursts of anger. We can improve patient outcomes and our work-life satisfaction by understanding why anger occurs, learning to become aware of what goes on in others' brains when they are upset, and adopting optimal techniques for handling these tough situations. Learning how to deal with difficult patients and being able to resolve conflict in a positive manner is one of the most valuable skills a nurse can possess.
Self Quiz
Ask yourself...
-
Think of an interaction you've had with a patient that was angry.
-
What was the outcome?
-
Was it positive, or could it have gone better?
Consider Anger
We all have our own personal opinions when it comes to understanding and tolerating anger in ourselves and others. Generally, it doesn't feel good to experience it, nor is it pleasant to be around others who are feeling this way. Experiencing anger is part of being human, it's normal, and as healthcare professionals, we must learn more about it so we are aware of how to deal with difficult patients. Perhaps approaching this from a philosophical standpoint will further help us to see beyond our patient’s immediate anger and we can work to develop a plan to resolve the conflict.
Anger as a Motivator
First off, anger can be motivating. Oftentimes, when we perceive that there is a problem that is causing harm or injustice - whether it is affecting ourselves, a patient, the barista at the corner coffee shop, the planet, whatever - it is often anger that pushes us to act. As a very basic (and optimistic) example, a patient might be angry about being stuck in the hospital. Optimally, the experience will bother them enough to want to follow all of the steps their physician provides them so that they do not have to be readmitted.
Catharsis
For some, the act of being angry can be cathartic. For example, when we feel angry and begin to shout or slam a door, it is actually a way of releasing that built up, negative energy. Some people achieve catharsis and release their anger in productive ways, such as exercising, talking with a friend or therapist, journaling, or cleaning. Once you have completed the action and released the anger that you had, you slowly begin to calm down (1).
If we don't release this energy over long periods of time, it can unfortunately cause physical harm. Anger increases heart rate, blood pressure (think MI or CVA), blood sugar, and intraocular pressure; it can lower our immune function and increase our risk of developing cancer; it also affects the digestive system; decreases bone density, and can also cause headaches and migraines. Being angry also negatively impacts our short-term memory, as well as the ability to make rational decisions (2). Applying therapeutic techniques can be a beneficial method of how to deal with difficult patients, as this can provide the opportunity to help them release some of the pent-up emotions they have before they cause physical harm.
Control
When learning how to deal with difficult patients, we must consider the relationship anger has with control. When a person is in our care, there is undoubtedly at least one major thing going on with them that they cannot control; otherwise, they would be at home. Being in a hospital setting removes all of the controlled variables that the patient has been accustomed to from their daily life (i.e. foods, who they come in contact with and at what time, etc.) and a common response to this change is anger in an attempt to regain control of the situation (1).
Stress & Trauma
There is a strong correlation between people who carry a lot of anger inside of them and stressful life events, particularly childhood trauma such as neglect and physical abuse. There's also an association between anger and psychiatric disorders such as bipolar disorder and borderline personality disorder. This is not surprising since many people with these and other psychiatric disorders experienced extreme stress and trauma in their youth (3).
I find that keeping these tidbits of information about anger in mind helps me with how to deal with difficult patients and allows me to maintain my own composure.
Explore Your Thoughts/Feelings/Opinions/Triggers
Self-awareness is extremely important when learning how to deal with difficult patients. Allowing ourselves to be aware of our own experiences, feelings, and triggers, understanding that they can influence how we respond to others in heated situations. For example, suppose you are someone who grew up in a household where you frequently experienced violence -- in that case, you might respond in an unexpected, unhelpful, and unprofessional way when exposed to angry behavior from others, such as shouting back. On the flip side, perhaps you grew up in a household where there was little to no conflict and you are unsure of how to properly respond when someone behaves angrily towards you. Maybe you have been judged harshly for your feelings and/or resulting actions, and consequently, judge others the same in turn.
Oftentimes we aren't aware of our own tendencies until we step back and intentionally evaluate them. Considering your own experiences, thoughts, judgments, and things that trigger you can help you to become aware of why you react to situations the way that you do. You'll then be more prepared to respond in a deliberate way when you next find yourself in a scenario with a disgruntled patient.
Self Quiz
Ask yourself...
- Have you ever gotten so upset that you made a bad decision?
- Has anger ever motivated you?
- What is your opinion of anger? How do you respond to others when they are angry?
- Think of at least three benefits of getting anger out.
Common Practice
"Calm down!" and, "It's not okay to yell!" yelled the nurse. We've all heard the countless ways healthcare professionals respond when figuring out how to deal with difficult patients who are angry. Maybe we have even found ourselves yelling similar statements as well, and that’s okay – we are all human, and being yelled at can be very triggering, Don't be too hard on yourself, evaluate how you should respond next time and prepare for it as best as you can because dealing with difficult patients is inevitable.
Often, clinicians become triggered - in other words, we get angry or irritated with ourselves when confronted with an angry patient. If we aren't mindful of our own tendencies and subsequently give in to that trigger, we inadvertently make what's going on with the patient about ourselves when the patient is the one who needs our care. How is it helpful if we become upset as well? When learning how to deal with difficult patients, keep in mind that by responding with anger or with words that are seeking to control, the patient will miss an opportunity to release their pent-up, intense energy which can result in physical harm.
I am reminded of a time when my daughter was an infant. She always had a terrible time facing backward in her car seat. We were riding with a friend of mine and her six-year-old son when my daughter began to cry. The young boy covered his ears, saying, "Why does she have to be so loud?" My friend's golden response was, "I know, honey, it's no fun, but think how much worse it must be for her."
Even though this scenario is quite different from a healthcare environment, I think those same words whenever I hear one of my patients yelling or are upset about something. All I want to do is cover my ears, but by thinking of how much worse it must be for them, I'm able to avoid making it about me.
Distraction
Another common approach to dealing with difficult patients during an angry episode is to utilize distraction. There are times when this application is going to be the best choice, particularly, when dealing with patients who are cognitively impaired (4). However, there are other instances where this technique may come off as insulting with otherwise oriented people and could exacerbate the issue.
An example of an appropriate time to utilize this technique would be when dealing with a patient who has dementia and gets increasingly (and repeatedly) worked up over their belief that a loved one - who hasn't seen the patient in recent history - is stealing from them. In this case, distraction might be the only way to calm them down.
Giving Advice
I work in a psychiatric setting, and when I was new to my position, I learned first-hand one technique that was not effective.
A 40-year-old, physically tall and sturdy male patient became so upset that he started punching our walls. Staff intervened and ending up having to take him down to the carpet for everyone's safety. Other than his increase in rate and depth of breathing, he was lying quietly, prone on the ground. I kept a safe distance and asked if he was alright: he didn't respond. I wasn't sure what to do or say. I was new, undoubtedly nervous, and hadn't yet learned the value of what one of our psychiatrists refers to as "therapeutic silence." I had learned in the past from my education and own personal experiences that breathing techniques were calming, so I tried saying, “it's okay, just breathe."
Subsequently, he began yelling at me. He was saying not to tell him what to do, that he hated me, and to go away. By suggesting something to him in that intense moment, he took offense. If I'm honest with myself, if I were upset and someone had said something similar to me, it might not have gone over much better.
Setting Limits
Although this should only be used when absolutely necessary, nurses must be able to learn and understand how to deal with difficult patients by setting limits to their behavior. Where I work, some patients simply live for the three smokes a day that they're allowed. An example of this sounds something along the lines of, "if you do not do XYZ, you're not going to get your cigarette." Please note that this approach should not be utilized all the time, but in some cases, it can seem like the only way to get through to your difficult patients.
Self Quiz
Ask yourself...
-
Can you think of other ways of handling patients who are angry?
-
What techniques have you employed?
-
How effective have they been?
Benefits of Learning How to Deal with Difficult Patients When They are Angry
As caregivers, we experience increased job satisfaction when we can adequately care for people who are angry. Imagine how rewarding it is to successfully manage situations and achieve positive outcomes for our patients that could've gone badly otherwise. Not only that but, we potentially run the risk of losing our jobs if we don't learn this essential skill (see Case Study #2 below). Rapport increases when appropriately utilized techniques are applied in practice because they foster trust and show respect for what the patient has to say (8).
For patients, these situations serve as great opportunities for them to release some of their anger. If we can be facilitators, assisting them to come to a more even-keeled place, they will undoubtedly experience better outcomes. Additionally, a situation involving a an angry patient can become dangerous quickly, so it is critical that we learn these skills for our own safety, and that of our patients.
Self Quiz
Ask yourself...
- Can you think of other benefits?
- Can you think of a time when a situation involving an angry patient became so much worse because of how it was handled?
Anatomy Review
The amygdalae are a couple of bunches of neurons found deep in each temporal lobe that play an important role in our emotions, including triggering the fight or flight response (5). The hypothalamus is near the base of the brain right under the thalamus, and is attached to the pituitary gland (6). Among many other things, it's responsible for controlling the secretion of hormones from the pituitary gland, which is located behind the nose (7). Finally, our adrenal glands sit on top of our kidneys and put out different kinds of hormones, particularly, stress hormones (2).
The Hormone Cascade
Something triggers us (i.e. we've just sat down to chart, and the call light goes off for what seems like the hundredth time, and we haven't eaten or used the bathroom all day). Our amygdalae, like canaries in a coal mine, sound the alarm by signaling the hypothalamus and release a corticotropin-releasing hormone -- causing the pituitary gland to release adrenocorticotropic hormone. This chain of hormone releases tells the adrenals to drop big stress bombs: adrenaline, noradrenaline, and cortisol (2).
When there's too much cortisol, increased calcium is allowed to get into our neurons, which can end up leading them to die. Our prefrontal cortex (PFC) and hippocampus suffer the most from this unfortunate outcome. The function of the PFC becomes suppressed, which affects our ability to have good judgment. For example, saying something hurtful or that you do not mean to someone you care about during an argument. Following, when neurons die in the hippocampus, this is where our memories are stored. So if it's not working well, our short-term memory and ability to store new ones are affected most (2).
The presence of too much cortisol will also result in a lack of serotonin - the happiness neurotransmitter. With less serotonin, we feel more sensitive to pain, anger, increase in aggression, and more prone to depression (2).
Consider every time you've ever tried to reason with a person who was already upset. How did it go? Did they immediately come to see the error of their ways? I can think of several occasions where a patient was so enraged about something that fixing whatever the issue was did nothing to quell the tirade. When trying to figure out how to deal with difficult patients, understanding what is going on in their brain during these episodes of rage can help us to make sense of it all and how to plan a deliberate, appropriate, and effective way to resolve the conflict.
Self Quiz
Ask yourself...
-
Have you ever experienced being so angry that you experienced an amygdala hijack? If so, would you have called yourself "reasonable" when you were in that state?
-
Consider the last time you dealt with someone who was angry in light of the above cascade of events. Does it make more sense now (if you weren't already aware of what happens)?
Tips for Handling Patients When They are Angry
Beyond this lesson, you will find several publications that discuss how to manage de-escalation during potentially dangerous situations. De-escalation involves maintaining a calm demeanor and avoiding attempts to control the patient. As a result, they feel respected, and the trust between the two of you builds. Every person and situation is different, so a certain amount of intuition is also essential in order to creatively develop solutions (9).
Safety First
Since we now know that during escalated, angry situations, our patient’s brains are not exactly functioning at full capacity so try your best to expect the unexpected. One moment, a patient can seem like the calmest, and most collected person in the world -- then they get triggered, and who knows what could happen?
With this in mind, the first thing we always have to consider is safety - for ourselves, the patient, and others nearby. Here are some recommendations for keeping everyone as safe as possible:
- Be aware of what's around you and your patient. Are there things that could be thrown or used as a weapon? Do you wear necklaces or long earrings that can be pulled?
- Always maintain a safe distance. If you don't feel safe, get to safety. It's okay to walk away from a situation if you feel that you are in danger, but never turn your back.
- Bring a co-worker if you need to go into an angry patient's room - never go alone.
- Observe for signs of aggression. If your patient exhibits balled fists, getting too close to you, pacing, tense shoulders, glaring, tense jaw, facial flushing, shouting, or heavy breathing, be prepared.
- Try to keep the area clear of others who might be put in danger or exacerbate the situation. This might be a challenge when you're focused on engaging with your patient. However, it is helpful if you and your coworkers are all on the same page. Consider working with management to train everyone to be on alert for potentially dangerous situations with patients and their loved ones.
What to Say vs. What Not to Say
When I'm upset, the thing that helps me the most is feeling like I am being heard. For my patients, I have found that listening is one of the tactics that works best, but remember that in some instances, patients may have a hard time listening to others because they may become triggered. If that occurs, it can become difficult to maintain a calm demeanor that is necessary for de-escalating tense situations. If we can find a way to keep the focus on the other patient (who is coming to us with the issue), we can become better listeners and remain calm.
Listening is a skill that not everyone excels in but it can make a huge difference when figuring out how to deal with difficult patients.
Tips to improve listening skills:
- Do not interrupt.
- Give your full attention rather than getting distracted by inner thoughts or environmental stimuli.
- Repeat back what you've heard to affirm you got it right.
- Ask related questions to show you're concerned and want to deepen your understanding.
- Convey a sense of empathy by using your body language, and making brief statements like, "That's understandable."
Since there is not a specific prescription or solution for dealing with all angry patients, we need to stay tuned and be creative to reach a mutually beneficial goal. By staying calm and truly listening, we're better able to understand what is going on so that we can attempt to remedy whatever the problem is when the time is right. After listening, affirming, and giving the patient time to calm down, we can begin to work toward a solution. For example, I might say, "I hear that you're upset about what happened, and that's totally understandable. What can I do for you right now to help?" By approaching the situation this way, it affirms that I heard the patient, respect their feelings, and genuinely want to help them. When learning how to deal with difficult patients, this is an extremely valuable tool to possess.
Additionally, body language is extremely important - it conveys so much! Simple adjustments like squaring ourselves to whomever we're listening to and conveying accurate facial expressions depending on the situation ensures in the patient that we are giving them our full, undivided attention and that we truly care about what they’re saying.
Boundaries
A word about maintaining boundaries; these are key! Just because I aim to listen and convey kindness actively does not mean that I am a pushover, and that my patients will get everything they want.
For example, as nurses, we all know that we often don't have the time (or energy) to have deep, confiding conversations with each and every patient. However, being kind can be done swiftly, and without caving to demands. A simple "no" can be said in a respectful manner. For example, we can briefly say in a kind tone, "I know it's frustrating, and I get it, but unfortunately, I can't talk with you right now because I'm in the middle of passing meds. Can we talk in half an hour or so?"
There are also times when we have to set boundaries because we can see that we can't do any good in that moment. I have a patient who shouts so loudly when they are upset that I have to cover my ears for fear of damage! Sometimes they are able to convey their feelings in a way that I can actively listen to, and these times seem to be helpful for them, but when they can't, I give them boundaries. I say, "I want to listen to you, but you're hurting my ears." If they are unable to control the volume, I gently remove myself, stating, "I hear that you're having a hard time, but I have sensitive ears, and your shouting is hurting them. Let's talk later."
We all have to figure out where our boundaries lie. If you are someone who gets triggered by the angry behavior of others, you might do best to excuse yourself early on to catch your breath and ask someone else to help with the situation. If you are triggered, it'll be tough for you to make the best decisions when figuring out how to deal with difficult patients.
Not Taking Things Personally
As nurses, I am sure we have all learned early on to not take anything personally, especially when dealing with difficult patients. In most cases, an angry patient yelling in your face will not be your fault. Remember, we are not responsible for other's feelings and reactions; those are about them, not us. As we mentioned previously, we are all probably guilty of saying something that we didn’t mean when we were upset and we wish we would have given it a second thought, and in some scenarios, this could be the case. However, there are other instances where the angry behavior of a patient then results in them wanting to speak with your manager regardless of whatever the reason is being your fault or not.
It's helpful to recognize when a behavioral response is not in proportion to what actually happened because this can be a clue into possible long-standing issues. Of course, knowing all of this doesn't mean we shouldn't always do our best, but it can help us refrain from beating ourselves up too much when our best seems to fall short.
Attempt to be aware of the things we have reviewed here so you can effectively handle and devise a solution on how to deal with difficult patients who are angry. Bear in mind how challenging it can be not to have control, especially during situations where we are unable to make rational decisions.
What to Do if You're the One to Lose Your Cool
As we discussed earlier, when we become triggered, our prefrontal cortexes (PFCs) don't work properly, and that is when our decision-making becomes poor. The good news is that, since we know what's going on in our brain, we can work on reactivating that precious (and potentially life-saving) PFC. At first, we might not be able to look at ourselves clearly until after an episode, but we can learn to recognize the signs of becoming triggered by examining what happened. Once we can do that in real-time, we can intentionally work toward becoming calm again.
Take Care of Yourself
Nurses are used to taking care of others all the time, but what about themselves? This is crucial. You must take care of and be kind to yourself. Our best is different every moment of every day, and that's all just part of being human. Some days, we might be having a tough time, struggling with any number of things, just like our patients. Our temper might be shorter, our tone may be a little more on edge, but rather than judging ourselves too harshly, we should recognize our own humanity and just do our best.
Self Quiz
Ask yourself...
- What kind of training have you received on safety? If none, is there an opportunity for growth in this area?
- List three things that help calm you if/when you get upset.
- Think of when you're listening to a patient. What do you do to show you're actively listening?
- What are some phrases you would feel comfortable saying that would show that you care and are actively engaged? (For example, "That sounds frustrating.")
Case Studies on How to Deal with Difficult Patients
Case Study #1
A 46-year-old female patient received an IM injection in her right glute this morning. It is afternoon shift change, and she is complaining that her right hip has been hurting since receiving this injection. She has repeatedly been approaching the nurse's station about this issue. The off-going day shift nurse calls over his shoulder as he's frantically attempting to finish documenting, "I've already assessed you, and I don't see anything wrong. I talked to the doctor, and he ordered Ibuprofen which you received. I have let her know that you would like to speak with her; you'll have to wait until she rounds next."
The patient begins yelling, stating, "None of you care about me! My doctor doesn't care about me! Otherwise, she wouldn't make me get these injections that hurt me!" The evening shift nurse arrives, sees that the patient she knew from the evening before is upset and that the off-going nurse is busy. The evening nurse steps behind the station desk so that there's a barrier between her and the patient (in case she becomes more agitated and aggressive) and turns to face the patient with a concerned expression in place. "*Fiona, I see that you're upset. How can I help?" The nurse listens, not interrupting the patient as she relays her issue. At a natural lull in the patient's speech, the nurse responds, "It sounds like you're frustrated about this situation. I get it; that's totally understandable." The patient goes on to express her feelings of not being cared for by the staff or the doctor, tearfully raising her voice. The nurse looks at the patient with concern and considers the possibility that this woman might have some history of not being cared for. She continues to listen as the patient goes on venting. Eventually, the patient shouts one last time, turns away, and stomps down the hall to her room. An hour later, she returns looking tired, a little embarrassed, but calm, and apologizes then thanks the nurse for listening.
Case Study #2
A 70-year-old male patient rings the call bell. The nurse answers and the patient shouts loud enough to be heard without the aid of the speaker, "Get over here! You people are useless! Because of you, I'm swimming in a puddle of my own urine." The nurse responds, "Okay, but you don't have to be so rude." The nurse slams the phone down, muttering expletives to themselves. They takes their time, finishing up what they were working on, still ruminating over the patient, while he gets increasingly upset.
They walks into the patient's room, and sees that he's standing next to his bed, naked, leaning precariously on his IV pole. The nurse says, "What are you doing? You're going to fall." The patient responds, "Well, you're not doing your job!" "I shouldn't have to deal with this," the nurse mutters under their breath as they begins to gather the soiled sheets. The nurse, whose back is turned to the patient, doesn't see that his face has gone the color of a bag of packed RBCs, his eyes are bulging, and his knuckles are white as they grip the IV pole. The patient attempts to use the pole as a weapon to hurt the nurse but ends up slipping on his urine-wet feet, striking his head against the wall, resulting in a concussion. He files an official complaint regarding the nurse, considers suing them for damages, and the nurse gets written up for the second time. Next time, they'll be out of a job.
Self Quiz
Ask yourself...
-
Think of one example from your practice that you have experienced or observed that went well and another that did not. What were the key elements that you think made the difference?
Conclusion
People get angry - it's just a fact of our existence. Some, unfortunately, make poor choices when they feel anger whether it's out of frustration, stress, feelings of loss of control, or unmanaged old triggers coming to the surface. As nurses, we often have to figure out how to deal with difficult patients while being able to remain calm and composed. By understanding more about people who experience excessive anger and learning to apply the techniques discussed in this course, you will be able to form flexible and creative solutions that can result in making the best out of very challenging situations.
References + Disclaimer
Key Concepts of Critical Thinking in Nursing
- Chan, Z. (2013, March 1). A systematic review of critical thinking in nursing education. Retrieved March 17, 2021, from https://www.sciencedirect.com/journal/nurse-education-today
- Lee, W., Chiang, C., Liao, I., Lee, M., Chen, S., & Liang, T. )2013, October 1). The longitudinal effect of concept map teachin on critical thinking of nursing students. Retrieved March 17, 2021, from https://pubmed.ncbi.nlm.nih.gov/22795871/https://doi.org/10.1016/j.nedt.2021.06.010
- Fesler-Birch, D. (2005, April 1). Critical thinking and patient outcomes: A review. Retrieved March 17, 2021, from https://pubmed.ncbi.nlm.nih.gov/15858523/
- Scriven, M., & Paul, R. (2007, January 1). Defining critical thinking. Retrived March 17, 2021, from https://www.criticalthinking.org/pages/defining-critical-thinking/766
- Zurmehly, J. The Relationship of Education Preparation, Autonmy, and Critical Thinking to Nursing Job Satisfacttion. The Journal of Continuing Education in Nursing. 2008;39(10):453-460
- Butler, H. (2012, June 20). Halpern critical thinking assessment predicts real-world outcomes of critical thinking. Retrieved March 17, 2021, from https://onlinelibrary.wiley.com/doi/pdf/10.1002/acp.2851
- Zori, S., Nosek, L., & Musil, C. (2010, July 08). Critical thinking of nurse managers related to staff RNs’ perceptions of the practice environment. Retrieved March 17, 2021, from https://pubmed.ncbi.nlm.nih.gov/20738741/
- Kaddoura, M. New graduate nurses’ perceptions of the effects of clinical simulation on their critical thinking, learning, and confidence. Journal of Continuing Education in Nursing, 41 (11) (2010), pp. 506-516
Effective Communication in Nursing
- Dictionary by Merriam-Webster: America’s most-trusted online dictionary. (n.d.). Retrieved February 22, 2021, from https://www.merriam-webster.com/
- Effects of poor communication in healthcare. (n.d.). Retrieved February 22, 2021, from https://www.hipaajournal.com/effects-of-poor-communication-in-healthcare/?amp
Ensuring Patient Confidentiality in Nursing
- American Nurses Association. (2015, June). American nurses association position statement on privacy and confidentiality. https://www.nursingworld.org/~4ad4a8/globalassets/docs/ana/position-statement-privacy-and-confidentiality.pdf
- Emergency Nurses Association. (2014). Sheehy’s manual of emergency care. In B. B. Hammond & P. G. Zimmermann (Eds.), Sheehy’s Manual of Emergency Care (7th ed., pp. 3–4). Elsevier Health Sciences.
- U.S. Department of Health & Human Services. (2015, November 6). Methods for De-identification of PHI. HHS.gov. https://www.hhs.gov/hipaa/for-professionals/privacy/special-topics/de-identification/index.html
- U.S. Department of Health & Human Services. (2013, July 26). Summary of the HIPAA Privacy Rule. HHS.gov. https://www.hhs.gov/hipaa/for-professionals/privacy/index.html
- U.S. Equal Employment Opportunity Commission. (2008). The Genetic Information Nondiscrimination Act of 2008 | U.S. Equal Employment Opportunity Commission. U.S. Equal Employment Opportunity Commission. https://www.eeoc.gov/statutes/genetic-information-nondiscrimination-act-2008
- Westrick, S. J. (2014). In Essentials of nursing law and ethics (2nd ed., pp. 77–84). Jones & Bartlett Learning.
Nursing Documentation 101
- 29-1141 Registered Nurses. (2018, March 30). Retrieved March 1, 2019, from https://www.bls.gov/oes/2017/may/oes291141.htm
- Hendrich, A., Chow, M. P., Skierczynski, B. A., & Lu, Z. (2008). A 36-hospital time and motion study: how do medical-surgical nurses spend their time?. The Permanente journal, 12(3), 25-34.
- Health IT Quick Stats. (2019, February 6). Retrieved March 1, 2019, from https://dashboard.healthit.gov/quickstats/quickstats.php
- Medical Practice Efficiencies & Cost Savings. (2018, August 13). Retrieved March 1, 2019, from https://www.healthit.gov/topic/health-it-and-health-information-exchange-basics/medical-practice-efficiencies-cost-savings
- Meaningful Use. (2017, January 18). Retrieved March 1, 2019, from https://www.cdc.gov/ehrmeaningfuluse/introduction.html
- Miller, L., Stimely, M., Matheny, P., Pope, M., McAtee, R. & Miller, K. Novice Nurse Preparedness to Effectively Use Electronic Health Records in Acute Care Settings: Critical Informatics Knowledge and Skill Gaps. (2014). Online Journal of Nursing Informatics,18(2). Retrieved March 1, 2019, from https://www.himss.org/novice-nurse-preparedness-effectively-use-electronic-health-records-acute-care-settings-critical
- HHS Office of the Secretary,Health Information Privacy Division. (2016, February 25). Individuals’ Right under HIPAA to Access their Health Information. Retrieved March 1, 2019, from https://www.hhs.gov/hipaa/for-professionals/privacy/guidance/access/index.html
- Office for Civil Rights (OCR). (2015, December 18). 2000-Why is the HIPAA Security Rule needed and what is the purpose of the security standards. Retrieved March 1, 2019, from https://www.hhs.gov/hipaa/for-professionals/faq/2000/why-is-hipaa-needed-and-what-is-the-purpose-of-security-standards/index.html
- AHIMA Work Group (2013). Integrity of the Healthcare Record: Best Practices for EHR Documentation (2013 update). Journal of AHIMA,84(8), 58-62. Retrieved March 1, 2019, from http://library.ahima.org/doc?oid=300257#.XHuU6YhKiUl
- What is Malpractice? (n.d.). Retrieved from https://www.abpla.org/what-is-malpractice#medical
- Cady, R. F., Esq. (2009). Criminal Prosecution for Nursing Errors. JONA’s Healthcare Law, Ethics, and Regulation,11(1), 10-16. Retrieved March 1, 2019, from https://www.nursingcenter.com/cearticle?an=00128488-200901000-00003&Journal_ID=260876&Issue_ID=848807
- Kann, B. R., Beck, D. E., Margolin, D. A., Vargas, D., & Whitlow, C. B. (Eds.). (2018). Improving Outcomes in Colon & Rectal Surgery. Retrieved March 1, 2019, from https://books.google.com/books?id=O61vDwAAQBAJ&dq=Improving Outcomes in Colon & Rectal Surgery edited by Brian R. Kann, David E. Beck, David A. Margolin, H. David Vargas, Charles B. Whitlow&source=gbs_navlinks_s
- Peters, P. G. (2008). Twenty Years of Evidence on the Outcomes of Malpractice Claims. Clinical Orthopaedics and Related Research, 467(2), 352-357. doi:10.1007/s11999-008-0631-7
- Singh, H. (2018). National Practitioner Data Bank Generated Data Analysis Tool. Retrieved March 1, 2019, from https://www.npdb.hrsa.gov/analysistool/
- Top 5 Malpractice Claims Made Against Nursing Professionals. (n.d.). Retrieved March 1, 2019, from https://www.proliability.com/portals/0/docs/nursemalpracticewhitepaper.pdf
- American Nurses Association. (2010). ANA’s Principles for Nursing Documentation. Retrieved February 28, 2019, from https://www.nursingworld.org/~4af4f2/globalassets/docs/ana/ethics/principles-of-nursing-documentation.pdf
- Lippincott Nursing Education. (2018, February 22). Lippincott Nursing Education Blog. Retrieved March 1, 2019, from http://nursingeducation.lww.com/blog.entry.html/2018/02/22/nursing_documentatio-S5hF.htmlOther references include:
- Reising, D. L., & Allen, P. N. (february 2007). Protecting yourself from malpractice claims. American Nurse Today,2(2). Retrieved March 1, 2019, from https://www.americannursetoday.com/protecting-yourself-from-malpractice-claims/.
- Reising, D. L. (2012). Make your nursing care malpractice-proof. American Nurse Today,7(1). Retrieved March 1, 2019, from https://www.americannursetoday.com/make-your-nursing-care-malpractice-proof/
Nursing Ethics
- Gallup Poll finds nursing is most honest and ethical profession. (2021, January). Oakland University News,, . https://oakland.edu/oumagazine/news/nursing/2021/gallup-poll-finds-nursing-is-most-honest-ethical-profession
- Rushton, C. (2017, January). Why ethics?. John Hopkins Nursing. https://magazine.nursing.jhu.edu/2017/01/why-ethics/
- Fowler, M., “Nursing’s Code of Ethics, Social Ethics, and Social Policy,” Nurses at the Table: Nursing, Ethics, and Health Policy, special report, Hastings Center Report 46, no. 5 (2016): S9-S12. DOI: 10.1002/ h
- Florence Nightingale Pledge. (2010) https://nursing.vanderbilt.edu/news/florence-nightingale-pledge/#:~:text=I%20solemnly%20pledge%20myself%20before,knowingly%20administer%20any%20harmful%20drug
- Rich, K., & Betts, J. (). Ethical theories and approaches. Jones & Bartlett Learning.
- The ICN Code of Ethics for Nurses (2021). https://www.icn.ch/system/files/documents/2020-10/CoE_Version%20for%20Consultation_October%202020_EN.pdf
- Edmonton, C. & Zelonka, C. (2019). My own worse enemy: the nurse bullying epidemic. Nursing Administration Quarterly. July – September. 43(3). 274-279.
- Bell, J.A. ( 2013). Five generations in the nursing workforce. Journal for Nurses in Professional Development 29( 4 ) https://www.sgna.org/Portals/0/Bell_FiveGenerationsInTheNursingWorkforce_2013.pdf
- Should Euthanasia Or Physician Assisted Suicide Be Legal(2019). https://euthanasia.procon.org/
- Llamas, J. V. (2018, November). The moral and ethical dilemma of physician assisted suicide. Minority Nurse, (), . https://minoritynurse.com/the-moral-and-ethical-dilemma-of-physician-assisted-suicide/
- 11. Lockwood, W. (2020, April). Jurisprudence and nursing ethics. http://file:///D:/Ethics%20in%20Nursing/Jurisprudence.pdf
Infection Control and Barrier Precautions
- RETRACTED: https://www.health.ny.gov/diseases/conditions/sepsis/
- https://www.health.ny.gov/facilities/public_health_and_health_planning_council/meetings/2013-02-07/docs/13-01.pdf
- RETRACTED: https://health.ny.gov/press/reports/docs/2017_sepsis_care_improvement_initiative.pdf
- https://www.sepsis.org/sepsis-basics/what-is-sepsis/
- https://www.nhsinform.scot/illnesses-and-conditions/blood-and-lymph/septic-shock
- Kim, H, & Park, S. (2019). Sepsis: Early recognition and optimized treatment. Tuberculosis and Respiratory Disease, 82(1), 6-14. doi: 10.4046/trd.2018.0041
- https://www.sccm.org/SurvivingSepsisCampaign/Guidelines/Adult-Patients
- https://www.mayoclinic.org/diseases-conditions/sepsis/diagnosis-treatment/drc-20351219
- https://www.cdc.gov/sepsis/pdfs/Consumer_fact-sheet_protect-yourself-and-your-family-P.pdf
PTSD in Nurses
- Torres, F. (2020, August). What is Post-traumatic Stress Disorder. Retrieved February 17, 2021, from https://www.psychiatry.org/
- DSM-5 Diagnostic Criteria for PTSD Trauma-Informed Care in Behavioral Health Sciences NCBI. (n.d.). Retrieved February 17, 2021, from https://www.ncbi.nlm.nih.gov/books/NBK207191/box/part_ch3box16/
- Posttraumatic Stress Disorder (PTSD): Patient Health Information. (n.d.). Retrieved February 17, 2021, from https://www.mayoclinic.org/diseases-conditions
- PTSD Examined: The five types of Post-traumatic Stress Disorders. (2020, August 26). Retrieved February 18, 2021, from https://bestdaypsych.com/ptsd-examined-the-five-types-of-post-traumatic-stress-disorder/
- What are the stages of PTSD. (2020, July 15). Retrieved February 18, 2021, from https://pyramidfbh.com/what-are-the-stages-of-ptsd/
- Mallvoire, B. L., Girard, T. A., Patel, R., & Monson, C. M. (2018). Functional connectivity of hippocampal sub regions in PTSD: Relations with symptoms. BMC Psychiatry, 18(129). https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-018-1716-9
- Brewin, C. R., Gregory, J. D., Lipton, M., & Burgess, N. (2010). Intrusive images in psychological disorders: characteristics, neural mechanisms, and treatment implications. Psychological Review,117(1), 210-232. https://pubmed.ncbi.nlm.nih.gov/20063969/
- Posttraumatic stress disorder in doctors. (2005, February 26). Retrieved February 18, 2021, from https://www.bmj.com/330/7489/s86
- Mealer, M. Burnham, E. L., Goode, C. J., Rothbaum, B. & Moss, M. (2009). The prevalence and impact of posttraumatic stress disorder and burnout syndrome in nurses. Depression and Anxiety, 26(12), 1118-1126. https://doi.org/10.1002/da.20631
- Watkins, L. E., Sprang, K. R., & Rothbaum, B. O. (2018). Treating PTSD: A Review of Evidence-Based Psychotherapy Interventions. Frontiers in Behavioral Neuroscience, 12(258). Retrieved February 28, 2021, from https://www.frontiersin.org/article/10.338/fnbeh.2018.00258
- Medications for PTSD. (2017, July 31). Retrieved March 01, 2021, from https://www.apa.org/ptsd-guideline/treatment/medications
- Gore, T. A. (2018, November 14). Posttraumatic Stress Disorder Medication. Retrieved March 01, 2021, from https://emedicine.medscape.com/article/288154-medication#3
- Rosinta, U., & Robiana, M. (2019, February). The Effects of Progressive Muscle Relaxation in Reducing Fatigue among Nurses in Mental Hospital. Indian Journal of Public Health Research & Development, 10(2), 289-295. Retrieved March 2, 2021 from https://www.web.b.ebscohost.com/abstract?direct=true&profile=ehost&scope=site&authtype=crawler&jml=09760245&AN=13
- US Department of Veterans Affairs, V. (2014, January 15). Stress Inoculation Therapy (SIT). Retrieved March 02, 2021, from https://www.ptsd.va.gov/apps/decisionaid/resources/PTSDDecisionAidSIT.pdf
Sexual Harassment Prevention
- Sexual harassment of female registered nurses in hospitals. M. K. Libbus, K. G. BowmanJ Nurs Adm. 1994 Jun; 24(6): 26–31.
- Sexual harassment of nurses: an occupational hazard? S. J. Finnis, I. Robbins J Clin Nurs. 1994 Mar; 3(2): 87–95.
- Sexual harassment in nursing. Robbins, I, Bender MP, Finnis SJ . Journal of advanced Nursing (1997) 25 (1) 163-9.
- Prevalence of sexual harassment of nurses and nursing students in China: A Meta-analysis of observational Studies. Liang-Nan Z, Qian-Qian Z, Ji-Wen Zhang, Li Lu, Feng-Rong An, Chee H, Gabor S, Fang-Yu, Teris C, Ligang C, Yu-Tao. International Journal of biological Sciences (2019). 15 (4) 749-756.
- 2019 Sexual harassment training. Office of executive inspector general for the agencies of Illinois governor (2019). Retrieved from https://www2.illinois.gov/eec/Documents/
- Ethics Act, 5 ILCS 430/5-65(b). Illinois state officials and employees ethics acts (2019). Retrieved from Ethics Act, 5 ILCS 430/5-65(b).
- Types of sexual harassment: everything you need to know. https://www.upcounsel.com/types-of-sexual-harassment (2020).
- Code of federal regulations. Title 29- labor. Guidelines on discrimination because of sex. https://www.govinfo.gov/content/pkg/CFR-2016-title29-vol4/xml/CFR-2016-title29-vol4-part1604.xml
- Facts about retaliation (2015). U.S. Equal Employment Opportunity Commission. Retrieved from https://www.eeoc.gov/laws/types/facts-retal.cfm
- RETRACTED What is sexual harassment? Illinois sexual harassment and discrimination helpline (2020). Retrieved from https://www2.illinois.gov/sites/sexualharassment/Pages/Definitions.aspx
Following a DNR: An Ethical Dilemma in Nursing
- Ethics. (2021). Retrieved from https://www.dictionary.com/browse/ethics
- ANA. (2021). Retrieved from Ethics and Human Rights: https://www.nursingworld.org/practice-policy/nursing-excellence/ethics/
- Dugdale, D. C. (2020, January 12). Do-not-resuscitate order. Retrieved from MedlinePlus: https://medlineplus.gov/ency/patientinstructions/000473.htm
Screening for Suicide Risk Factors in Pediatrics
- American Foundation for Suicide Prevention (n.d.) Suicide prevention resources. Retrieved on March 12, 2021 from https://afsp.org/suicide-prevention-resources.
- Gordon, M. & Melvin, G. (2014). Risk assessment an initial management of suicidal adolescents. Australian Family Physician, 43(6), 367-372. Retrieved on March 12, 2021 from https://www.racgp.org.au/afp/2014/june/suicidal-adolescents/.
- National Institute of Mental Health (n.d.). Ask Suicide-Screening Questions (ASQ) Toolkit. Retrieved on February 19, 2021 from https://www.nimh.nih.gov/research/research-conducted-at-nimh/asq-toolkit-materials/index.shtml.
- Pasold, T. (2018). Suicide Screening in Adolescents. Arkansas Children‘s Hospitals Research Foundation. Retrieved on March 12, 2021 from https://www.archildrens.org/-/media/Files/for-healthcare-professionals/pediatric-guidelines/Suicide_Screening_in_Adolescents.pdf.
- Patterson S. (2016). Suicide Risk Screening Tools and the Youth Population. J Child Adolesc Psychiatr Nurs, 29(3):118-26. doi: 10.1111/jcap.12148. Epub 2016 Aug 23. PMID: 27552927. Retrieved on March 12, 2021 from https://pubmed.ncbi.nlm.nih.gov/27552927/.
Human Trafficking
- https://polarisproject.org
- https://humantraffickinghotline.org/state/michigan
- https://www.dhs.gov/blue-campaign/what-human-trafficking
- United Nations Office on Drugs and Crime. (2016). Global report on trafficking in persons, 2014. New York, NY: United Nations.
- https://www.justice.gov/humantrafficking/what-is-human-trafficking
- https://www.cdc.gov/violenceprevention/sexualviolence/trafficking.html
- https://polarisproject.org/2019-us-national-human-trafficking-hotline-statistics/
- https://polarisproject.org/wp-content/uploads/2019/09/LGBTQ-Sex-Trafficking.pdf
- Hachey, L., & Phillippi, J. (2017). Identification and management of human trafficking victims in the emergency department. Advanced Emergency Nursing Journal, 39(1), 31–51.doi: 10.1097/TME.0000000000000138
- RETRACTED:https://swmihumantrafficking.org/michigans-human-trafficking-law/
- Mandatory Reporting of Human Trafficking: Potential Benefits and Risks of Harm. AMA Journal of Ethics. Accessed d12/10/2020. https://journalofethics.ama-assn.org/article/mandatory-reporting-human-trafficking-potential-benefits-and-risks-harm/2017-01
- https://humantraffickinghotline.org/what-human-trafficking/federal-law
- RETRACTED: https://www.michigan.gov/mdhhs/0,5885,7-339-73971_7119_50648_44443-157836–,00.html
- Update: Identifying human trafficking patients alert. Patient Safety Monitor Journal. 2018;19(9):6. Accessed October 31, 2020. http://search.ebscohost.com /login.aspx?direct=true&db=ccm&AN=131246408&site=eds-live
- Identifying Victims of Human Trafficking: What to Look for in a Healthcare Setting. Journal of Legal Nurse Consulting. 2020;31(3):30-33. Accessed October 31, 2020. http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=145452392&site=eds-live
- https://www.state.gov/identify-and-assist-a-trafficking-victim/
- National Human Trafficking Hotline. Comprehensive human trafficking assessment tool. Retrieved from https://humantraffickinghotline.org/sites/default/files/Comprehensive%20Trafficking%20Assessment.pdf
- https://www.acf.hhs.gov/sites/default/files/orr/fact_sheet_sex_trafficking.pdf
Pain Management in Nursing
- https://www.cdc.gov/nchs/products/databriefs/db390.htm
- Institute of Medicine. (2011). Relieving pain in America: A blueprint for transforming prevention, care, education, and researchpdf iconexternal icon. Washington, DC: National Academies Press
- https://www.merriam-webster.com/dictionary/pain
- Nahin, R. (2012). Estimates of pain prevalence and severity in adults: United States. Journal of Pain, 16(8), 769-80. doi: 10.1016/j.jpain.2015.05.002
- Yam, M., Loh, Y., Tan, C., Adam, S., Manan, N., & Basir, R. (2018). General pathways of pain sensation and the major neurotransmitters involved in pain regulation. International Journal of Molecular Sciences, 19(2164), 1-23. doi: 10.3390/ijms19082164
- Swift, A. (2018). Understanding pain and the human body’s response to it. Nursing Times, 114(3), 22-26. Retrieved from https://www.nursingtimes.net/clinical-archive/pain-management/understanding-the-effect-of-pain-and-how-the-human-body-responds-26-02-2018/
- https://www.cdc.gov/media/releases/2016/p0315-prescribing-opioids-guidelines.html
- https://www.michigan.gov/document/lara/LARA_DHHS_Opioid_Laws_FAQ_05-02-2018_622175_7.pdf
- https://healthteam.msu.edu/patients/Policies-Forms/opioid-laws-FAQ.aspx
- https://www.michigan.gov/opioids/0,9238,7-377-88143_88345—,00.html
- Griesler, P., Hu, M., Wall, M., & Kandel, D. (2019). Medical use and misuse of prescription opioids in the US adult population: 2016-2017. American Journal of Public Health, 109(9), 1258-65. doi: 10.2105/AJPH.2019.305162
- https://www.michigan.gov/mdhhs /0,5885,7-339-71550_2941_4871_79584—,00.html
- Mills, S., Nicolson, K., & Smith, B. (2019). Chronic pain: a review of its epidemiology and associated factors in population-based studies. British Journal of Anesthesiology, 12(2), 273-283. doi: 10.1016/j.bja.2019.03.023
- Dahan, A., Velzen, M., & Niesters, M. (2014). Comorbidities and the complexities of chronic pain. Anesthesiology, 121(4), 675-677. doi: 10.1097/ALN.0000000000000402
- https://www.mhanational.org/chronic-pain-and-mental-health
- Mir, H. Miller, A., Obremskey, W., Jahangir, A. & Hsu, J. (2019). Confronting the opioid crisis: practical pain management and strategies. The Journal of Bone and Join Surgery, 101(23), 1-6. doi: 10.2106/JBJS.19.00285
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Fifth edition. 2014.
- Wardhan, R., & Chelly, J. (2017). Recent advances in acute pain management: understanding the mechanisms of acute pain, the prescription of opioids, and the role of multimodal pain therapy. F1000 Research, 6(2065), 1-10. Doi:10.12688/f1000research.12286.1
- https://static.practicalpainmanagement.com/sites/default/files/pain-management-medications.pdf
- https://www.cdc.gov/drugoverdose/training/nonopioid/508c/
- Ackley, B. J., Ladwig, G. B., Msn, R. N., Makic, M. B. F., Martinez-Kratz, M., & Zanotti, M. (2019). Nursing Diagnosis Handbook E-Book: An Evidence-Based Guide to Planning Care. Mosby.
- Hemmatipour, A., Karami, F., Sadouni, Z, Hatami, A., Jahanirmehr, A. & Saberipoiur, B., (2020). A comparison between nurses’ and patients’ views on barriers to pain management. Journal of Nursing and Midwifery Sciences, 2018(5), 47-52. Doi: 10-4103/JNMS.JNMS_16_18
- https://www.jointcommission.org/media/tjc/newsletters /quick_safety_drug_diversion_final2pdf.pdf
Drains: Everything you need to know
- Makama, J. G., & Ameh, E. A. (2008). Surgical drains: What the residents need to know. Nigerian Journal of Medicine: Journal of the National Association of Resident Doctors of Nigeria, 17(3), 244-50. doi: 10.4314/njm.v17i3.37389
- Knowlton, M. C. (2015). Nurse’s guide to surgical drain removal. Nursing 2015, 45(9), 59-61. doi: 10.1097/01.NURSE.0000470418.02063.ca
- Lemone, P., & Burke, K. (2008). Medical-surgical nursing(4th ed.). Upper Saddle, New Jersey: Pearson.
- Percutaneous. (2019). In Merriam-Webster Dictionary Online. Retrieved from https://www.merriam-webster.com/dictionary/percutaneous#medicalDictionary
- Wallace, M. J., Chin, K. W., Fletcher, T. B., Bakal, C. W., Cardella, J. F., Grassi, C. J., … Kundu, S. (2010). Quality improvement guidelines for percutaneous drainage/aspiration of abscess and fluid collections. Journal of Vascular and Interventional Radiology, 21(4), 431-435. doi: https://doi.org/10.1016/j.jvir.2009.12.398
- Hearns, W. C. (2012). Abscess drainage. Seminars in Interventional Radiology, 29(4), 325-336. doi 10.1055/s-0032-1330068
- Rivera-Sanfeliz, G. (2008). Percutaneous abdominal abscess drainage: A historical perspective. American Journal of Roentgenology, 191(3), 642-643. doi: 10.2214/AJR.07.3903
- Cinat, M. E., & Wilson, S. E. (2002). Determinants for successful percutaneous image-guided drainage of intra-abdominal abscess. Arch Surg., 137(7), 845-849. doi:10.1001/archsurg.137.7.845
- Lorenz, J. & Thomas, J. L. (2006). Complications of percutaneous fluid collection. Seminars in Interventional Radiology, 23(2), 194-204. doi: 10.1055/s-2006-941450
- National Institutes of Health. (n.d.) Patient education: How to care for the Jackson-Pratt drain. Retrieved from https://www.cc.nih.gov/ccc/patient_education/pepubs/jp.pdf
- St. Jude Children’s Research Hospital. (2019). Caring for a pigtail drain. Retrieved from https://www.stjude.org/treatment/patient-resources/caregiver-resources/patient-family-education-sheets/home-care-guidelines/caring-for-a-pigtail-drain.html
- (Image) Doyle, G. R., & McCutcheon, J. A. (2015). Clinical Procedures for Safer Patient Care. Victoria, BC: BCcampus. Retrieved from https://opentextbc.ca/introductiontosociology2ndedition/.
- Patel IJ, Davidson JC, Nikolic B, Salazar GM, Schwartzberg MS, Walker TG, Saad WA; Standards of Practice Committee, with Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Endorsement. Consensus guidelines for periprocedural management of coagulation status and hemostasis risk in percutaneous image-guided interventions. J Vasc Interv Radiol. 2012 Jun;23(6):727-36. do: 10.1016/j.jvir.2012.02.012. Epub 2012 Apr 17. PMID: 22513394.
- Mamuyac, E. M., Pappa, A. K., Thorp, B. D., Ebert, C. S., Jr, Senior, B. A., Zanation, A. M., Lin, F. C., & Kimple, A. J. (2019). How Much Blood Could a JP Suck If a JP Could Suck Blood? The Laryngoscope, 129(8), 1806–1809. https://doi.org/10.1002/lary.27710
Administration of Blood Products
- American Assoc. of Blood Banks, American Red Cross, America’s Blood Center, & Armed Services Blood Program. (2017, October). Circular of information for the use of human blood and blood components. Retrieved February 10, 2021, from https://www.aabb.org/docs/default-source/default-document-library/resources/circular-of-information-10-17.pdf.
- American Red Cross. (2020). Blood needs & blood supply. Retrieved February 10, 2021, from https://www.redcrossblood.org/donate-blood/how-to-donate/how-blood-donations-help/blood-needs-blood-supply.html.
- American Red Cross. (2017). A Compendium of Transfusion Practice Guidelines Edition 3a. Retrieved from https://www.redcrossblood.org/content/dam/redcrossblood/documents/249301_compendium_v03.pdf.
- Barnhard, C., Howell, E., Tran, N., Flanders, S., & Rosenthal, M. (2020, January). “This is the wrong patient’s blood!”: Evaluating a near-miss wrong transfusion event. Retrieved February 10, 2021, from https://psnet.ahrq.gov/web-mm/wrong-patients-blood-evaluating-near-miss-wrong-transfusion-event#:~:text=The%20most%20frequent%20error%20leading,other%20than%20the%20correct%20recipient.
- Center For Disease Control and Prevention. (2020, March 18). Blood safety BASICS. Retrieved February 10, 2021, from https://www.cdc.gov/bloodsafety/basics.html#anchor_1548882314
- The Joint Commission. (2020). National Patient Safety Goals Effective January 2020 [Brochure]. Oakbrook Terrace, IL. Retrieved from https://www.jointcommission.org/- goals/2020/npsg_chapter_hap_jan2020.pdf?db=web&hash=6CC50D956B7AC5CF6BD2 2BDB7577B5A0
A Nurse’s Guide: How to Deal with Difficult Patients
-
Ratson, M. (2017, March 09). The value of ANGER: 16 reasons it’s good to get angry. Retrieved February 17, 2021, from https://www.goodtherapy.org/blog/value-of-anger-16-reasons-its-good-to-get-angry-0313175
-
National Institute for the Clinical Application of Behavioral Medication. (2020, August 28). How anger affects the brain and body [infographic]. Retrieved February 18, 2021, from https://www.nicabm.com/how-anger-affects-the-brain-and-body-infographic/
-
Okuda, M., Picazo, J., Olfson, M., Hasin, D., Liu, S., Bernardi, S., & Blanco, C. (2015, April). Prevalence and correlates of anger in the community: Results from a national survey. Retrieved February 19, 2021, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4384185/
-
Brooker, C. (2017, July). Communication with angry patients through de-escalation. Retrieved February 18, 2021, from https://www.elsevierclinicalskills.co.uk/SampleSkill/tabid/112/sid/1727/Default.aspx
-
Moyer, N. (2019, April 22). Amygdala hijack: What it is, why it happens and how to make it stop. Retrieved February 18, 2021, from https://www.healthline.com/health/stress/amygdala-hijack#overview
-
Seladi-Schulman, J. (2018, March 21). Hypothalamus: Anatomy, function, diagram, conditions, health tips. Retrieved February 18, 2021, from https://www.healthline.com/human-body-maps/hypothalamus
-
Seladi-Schulman, J. (2018, June 11). Pituitary gland overview. Retrieved February 18, 2021, from https://www.healthline.com/health/human-body-maps/pituitary-gland
-
Awdish, R., & Berry, L. (2017, October 13). The importance of making time to really listen to your patients. Retrieved February 24, 2021, from https://www.physicianleaders.org/news/the-importance-of-making-time-to-really-listen-to-your-patients#:~:text=Actively%20listening%20conveys%20respect%20for,to%20truly%20listen%20to%20patients
-
Price, O., & Baker, J. (2012). Key components of de-escalation techniques: A thematic synthesis. Retrieved February 25, 2021, from https://www.researchgate.net/profile/Owen-Price-2/publication/221837683_Key_components_of_de-escalation_techniques_A_thematic_synthesis/links/5a1e8b21458515a4c3d1faa0/Key-components-of-de-escalation-techniques-A-thematic-synthesis.pdf
Disclaimer:
Use of Course Content. The courses provided by NCC are based on industry knowledge and input from professional nurses, experts, practitioners, and other individuals and institutions. The information presented in this course is intended solely for the use of healthcare professionals taking this course, for credit, from NCC. The information is designed to assist healthcare professionals, including nurses, in addressing issues associated with healthcare. The information provided in this course is general in nature and is not designed to address any specific situation. This publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals. Hospitals or other organizations using this publication as a part of their own orientation processes should review the contents of this publication to ensure accuracy and compliance before using this publication. Knowledge, procedures or insight gained from the Student in the course of taking classes provided by NCC may be used at the Student’s discretion during their course of work or otherwise in a professional capacity. The Student understands and agrees that NCC shall not be held liable for any acts, errors, advice or omissions provided by the Student based on knowledge or advice acquired by NCC. The Student is solely responsible for his/her own actions, even if information and/or education was acquired from a NCC course pertaining to that action or actions. By clicking “complete” you are agreeing to these terms of use.
➁ Complete Survey
Give us your thoughts and feedback
➂ Click Complete
To receive your certificate