Course
NY Identification and Reporting of Child Abuse and Maltreatment
Course Highlights
- In this NY Identification and Reporting of Child Abuse and Maltreatment course, you will learn how to determine if a child shows indicators of maltreatment or abuse, including in a virtual setting.
- You’ll also learn to recognize when a mandated reporter has the legal obligation to call the SCR.
- You’ll leave this course able to explain the main points of the legislation that pertains to the rights of mandated reporters.
About
Contact Hours Awarded: 2
Course By:
Sarah Schulze
MSN, APRN
Begin Now
Read Course | Complete Survey | Claim Credit
Pre-Evaluation
Please complete the evaluation below prior to reading any of the course material.
➀ Read and Learn
The following course content
Introduction
Child abuse and neglect happen across the country, affecting 1 in 7 children in the United States each year. Among the states with the highest rates of child abuse is New York, with an annual rate of abuse double that of the national average. In addition to this gut-wrenching statistic, the actual occurrence of abuse is believed to be underreported. The purpose of this course is to provide education to mandated reporters about risk factors, recognition, and reporting of abuse and to hopefully increase awareness of this tragic problem and reduce the number of children who are victims of harm.

Self-Quiz
Ask Yourself...
- Why do you feel that New York has such a high incidence of child abuse compared to other areas?
- What factors do you think cause the occurrence of child abuse to be underreported?
- Do you think burnout can cause you to be less alert to the signs of child abuse?
- Do you feel like the incidence of child abuse has been increasing or decreasing in your workplace?
- What biases do you have that have impacted your practice when dealing with incidences of abuse?
New York State’s Child Welfare Practice Model
Excerpt from the CPS Manual (12)
“New York State’s Child Welfare Practice Model establishes a consistent and recognizable approach to child welfare practice across New York State. Children, families, and adults are protected and supported to achieve safety, permanency, and well-being.
The Practice Model is founded on these values:
- We believe children and adults have the right to be safe, and to have permanent families and lasting relationships.
- We listen first, then learn and proceed with knowledge, focusing on the individual and family resources and strengths.
- We believe that services for children, families, and adults must be individualized and culturally competent, recognizing, and honoring differences in traditions, heritage, values, and beliefs.
- We approach our work with a sense of urgency and persistence, recognizing and respecting a child and family’s sense of time.
- We believe that high-performing supervisors and caseworkers are key to building and sustaining an effective child welfare system.
- We value interagency collaboration.
- We believe in accountability for action and results.
- We strive for data-informed decision-making.
- We value the principles of partnership:
- Everyone desires respect.
- Everyone needs to be heard.
- Everyone has strengths.
- Judgments can wait.
- Partners share power.
- Partnership is a process.”
Epidemiology- Current Patterns of Abuse in New York
Every year across the United States, nearly 700,000 children are abused or neglected in families of all racial, ethnic, and socioeconomic backgrounds. Abuse and neglect encompass many situations that cause physical, mental, or emotional harm through intentional acts of maltreatment or failing to meet a child’s basic needs to the point of endangering their overall health and well-being (8).
Any person under the age of 18 can be a victim of child abuse, but very young children are most at risk, and abuse commonly occurs during the first 2 years of life when they are not yet highly verbal. Nationally, around 75% of deaths from child abuse occur in children under the age of 3. Children are affected nearly equally across genders. The abuser is a parent or guardian over 78% of the time (1).
Neglect is the most common form of abuse, accounting for 60.8% of confirmed abuse cases nationally. Physical abuse accounts for 10.7% of cases, sexual abuse occurs 7% of the time, and emotional/psychological abuse occurs 2.3% of the time. Often, children experience two or more types of abuse (8).
The occurrence of abuse varies by state, and unfortunately, New York leads by nearly double the national rate of child abuse, with 17 children per 1,000 being the victim of some form of abuse in 2017. Even the New York County with the lowest rate of abuse, Saratoga, with 12.7 children per 1,000 affected, is still over 3 points higher than the national average. The worst county in the state is Montgomery, with a staggering rate of 34.3 children per 1,000 (10).
A 2017 analysis from the Child Welfare League of America identified 156,994 reports of child abuse and neglect in New York and reported that over 20,000 children were living separately from their families due to removal from the home following abuse or neglect (5).
The effects of child abuse are far-reaching; in addition to the obvious physical injuries and health problems, childhood victims of abuse are more likely to suffer from psychological issues such as anxiety, depression, chronic fear, and difficulty forming intimate relationships for the rest of their lives. Behavioral problems such as poor academic achievement, substance abuse, crime, teen pregnancy, and delinquency are increased in abuse victims as well, and the state of New York spends an estimated $2.4 billion per year on child welfare, law enforcement, and healthcare-related costs (9).
Self-Quiz
Ask Yourself...
- Think about the population you work with. Who is most at risk?
- What factors put young children at such a high risk of abuse?
- Consider the long-term effects of abuse on children. Why do you think people who have been victims of abuse as children are more likely to abuse their own children?
- How can a child’s change in environment cause an increased risk of abuse?
- What information about came as a surprise to you?
Defining Child Abuse and Neglect
To be an effective mandated reporter in the state of New York, you must have a clear understanding of who is involved in a child abuse situation and what is considered abuse or neglect. Abuse and neglect/maltreatment do have differing criteria, but it is up to the caseworker to investigate the report to determine where each situation falls. As a mandated reporter, you just need to know what sorts of scenarios warrant reporting, and the investigators will take care of the rest.
Definitions of particular importance include:
Child
A child is any individual after birth and up to the age of 18. Individuals under age 21 with certain disabilities who live in New York residential care facilities are also considered children under New York law (6).
Perpetrator
A perpetrator is anyone over the age of 18 who has been legally entrusted with the care of a child or children and knowingly causes harm to them through their actions or inactions. Most often, a perpetrator is a parent or legal guardian, but they can also include other relatives who live in the home, regular babysitters or nannies, or foster parents.
Individuals who cause harm to a child but are not legally responsible for their care are liable for different types of criminal charges but cannot be the subjects of a report. In the state of New York, this most often includes people like teachers or church personnel (6).
Abuse
Abuse is when a perpetrator inflicts or knowingly allows another person to inflict physical harm onto a child, causing serious injury or risk of death. This can include but is not limited to injuries such as burns, head trauma, fractures, or internal organ damage. It can also be considered an abusive situation if a person creates an environment that puts the child at great risk of serious injury or death, even if serious injury or death do not occur. Sexual acts are also included, such as rape, forcible touching, genital mutilation, or promoting or forcing sexual performance by a child (6).
Neglect and Maltreatment
Perhaps less immediately or life-threateningly dangerous, but still reportable, are neglect and maltreatment situations, which include:
- Anything that impairs (or risks impairment of) a child’s physical, mental, or emotional wellbeing.
- A failure to provide minimal standards of care such as food, shelter, clothing, medical attention, schooling, or supervision.
- Infliction of corporal punishment
- Creating an environment that is unsafe or unable to meet a child’s needs due to the misuse of drugs or alcohol by the parent or guardian.
- Abandonment (6)
It should be noted that physical discipline is legal in New York and that reports are only required for excessive or corporal punishment. Discipline is considered excessive or corporal punishment if it is severe or brutal, inappropriate for a child’s age/size, degrading to the child, outlasting a child’s endurance, or gratifying a parent’s rage (6).

Self-Quiz
Ask Yourself...
- Have you ever cared for a child who was a victim of abuse or neglect? What category did their situation fall under?
- Why might neglect or maltreatment be less obvious or more difficult to detect than abuse?
- What symptoms of abuse are easier to identify?
- What symptoms of abuse are more challenging to identify?
Identifying Child Abuse and Neglect
In addition to understanding what constitutes child abuse or neglect, mandated reporters need to be able to identify common signs or indicators that abuse has occurred or is occurring. Sometimes, abuse may be obvious and unquestionable; more often, however, the situation will be more subtle and require you to notice several indicators and combine them with your professional expertise.
There are three main types of indicators to be aware of, discussed below:
Child’s physical indicators
These indicators include bruises, fractures, lacerations, and other injuries to a child’s body that are inconsistent with typical childhood injuries or likely to require intentional force to occur. The location, size, and shape of bruises are important to consider; children commonly have bruises to bony prominences like elbows, knees, and shins from running and playing. Bruises over soft tissue like the buttocks, back, or the face and neck or bruises with clearly outlined shapes of a hand or household object are less common with typical play and are more suspicious. The types and mechanism of injury will vary with age. A child’s development should be considered and compared with the story of how an injury occurred and what types of injuries are likely to be accidental versus intentional. Also, pay close attention to children who have poor hygiene, dirty clothing, are always hungry, or frequently tired (2).
Child’s behavioral indicators
Do not assume that children will tell you if they are in an abusive situation. Often, children are afraid of retaliation from their abusers and will not report abuse to an adult, or they are too young to communicate or don’t even know that they can ask for help. You will need to be in tune with a child’s behavior in relation to their development and understand what behaviors raise suspicion for abuse. Children who are wary of adults (outside of the normal separation anxiety phase around 9-18 months), frequently falling asleep in class, hoarding or stealing food, behavioral regressions (toileting accidents, thumb sucking, etc.), change in sleeping or eating habits, withdrawn or overly quiet, anger or aggressive outbursts, delinquency, and drug abuse are all among behaviors to consider as potential red flags (2).
Virtual Settings
This is specific for providers or teachers that provide services to children through telehealth. Most of the signs will be the same, but you will have to be more intentional in your questioning and use critical thinking since sometimes you may have less one-on-one time with a child than in a face-to-face setting.
Other things to consider:
- Does the child frequently miss class/appointments because of a lack of internet or limited access to technology?
- Are they afraid to speak when their parent/caregiver is around?
- Attempts to reach parent/caregiver go unanswered.
- You hear yelling or screaming in the household.
- There is evidence that there may be illicit drug or alcohol use in the home and that the parents or even child are under the influence, etc. (14).
Perpetrator’s behavioral indicators
Attention must also be given to the behavior of the adult who is suspected of inflicting the abuse. Inconsistent stories or details of how an injury occurred, lack of concern for or delay in seeking care for a child’s injuries, talks negatively about the child (such as bad, mean, evil, etc.) are all suspicious for abuse. Consideration must also be given to a personal history of the parent of mental illness, substance abuse, or being abused as a child themselves. In general, if a story is not very believable or keeps changing, it should be regarded with a high amount of suspicion (2).
In any situation where you notice some of the above indicators or a child or parent gives you suspicious information, or your own clinical judgment raises concern, you have reasonable cause to suspect and are required to make a report. It is important to note that you do not have to have proof and that your own mistrust of a situation is enough to make a report in good faith. Even if you think or know another person has made a report regarding the same scenario, you still need to make your own report. This may not only help build a case against a potential abuser but may also offer a different perspective or additional information that others have not yet reported (9).
Whenever you suspect abuse or neglect, it may often be helpful to have a conversation with the child, if they are old enough, to gather more information. Remember that you are just trying to gather more information to add to your current assessment, but not trying to interrogate the child or investigate beyond the issue in front of you. When talking with children, be open and honest, let them know you are there to help, find a private place for the conversation, and listen while remaining calm. Particularly in the case of sexual abuse, it may be difficult or traumatizing for children to relive the details and so keep your conversation brief and to the point (2).
Case Study
A 6-year-old child is brought to the pediatrician for a wellness check. While the nurse is gathering vitals on the child, the mother apologizes for all of the bruises on the child’s shins and states she doesn’t even know how he got them. The child laughs and says he falls off his bicycle sometimes.
Self-Quiz
Ask Yourself...
- Is this situation presented in the case study concerning abuse? Why or why not?
- How can children be abused in a virtual setting?
- What child behaviors may indicate that they are enduring events?
- What physical indicators may present in a child being abused?
- What behaviors by a caregiver may indicate that they are abusing their child?
New York Child Protective Services
New York passed its Child Protective Services Act in 1973 which standardized criteria for the reporting and handling of investigations of child abuse and made these regulations into statewide law (10).
The main regulations outlined by this act include:
- Definition of a mandated reporter, duties of mandated reporters, and a detailed list of professions that fall under this mandate. This list is updated regularly.
- Creation of the State Central Register (SCR), a 24/7 statewide program operated by the New York State Office for Children and Family Services that receives reports of child abuse and neglect and passes them on appropriately.
- Establishment of local Child Protective Service (CPS) departments that receive registered reports from SCR and delegate them to CPS officers who investigate and handle the allegations from there (11).
The purpose of the CPS Act is to create a reliable and smoothly operating process for suspected abuse to be reported, documented, and investigated in the hopes of properly identifying abuse cases and preventing further harm from coming to affected children. It also helps to connect children, abusers, and family units with the resources needed to properly rehabilitate them and minimize long-term healthcare outcomes (11).
Self-Quiz
Ask Yourself...
- Why is a statewide protocol for reporting abuse allegations necessary?
- Additionally, why do you think investigation and action on reports is delegated to the local level?
Role of Mandated Reporters
So, what exactly is a mandated reporter, and who falls under this definition?
Anyone who witnesses or suspects abuse at any time may report it, but there are certain professional capacities that require a person to report any suspected abuse with the goal of keeping children as safe as possible and minimizing overall harm; these are mandated reporters. A comprehensive list is included in section 413 of the Social Services Law and is updated periodically.
In general, professions that are likely to come in contact with children or be at least somewhat responsible for the wellbeing of children, and are therefore mandated reporters, include (9):
- Healthcare workers- doctors, nurses, NPs, PAs, dentists, etc.
- School personnel- teachers, social workers, guidance counselors, administrators, school nurses, etc.
- Childcare or children’s program personnel- Daycare providers, church employees, camp counselors, etc.
Law enforcement and legal professionals- police officers, investigators, attorneys, etc.
When to Call the Statewide Central Register (SCR)
A comprehensive list is included in section 413 of the Social Services Law and is updated periodically. Those professionals who fall under the definition of mandated reporters are required to make a report to SCR any time that they are operating in a professional capacity and encounter a child they have reasonable cause to suspect is being maltreated.
The same requirement also applies any time a mandated reporter encounters someone they believe may be abusing a child or endangering them. Reports should be made immediately once suspicions arise. Mandated reporters are not required to report potential abuse scenarios they encounter when they are not working, though they would still be encouraged to report the incident on a “non-mandated” basis (9).
Case Study
Imagine you are a nurse working in an ED setting. Your patient is a 32-year-old woman who presents with a migraine. She brings her 4-year-old child with her until the child’s father can pick him up. The child is withdrawn, and the mother seems to have a poor attachment to him. She belittles him and tells him she wouldn’t get headaches and have to go to the hospital if he wasn’t such a bad kid. At one point, you note a large fading bruise on the back of his right arm. The father comes to pick up the child, and you continue on with the mother’s care.
Self-Quiz
Ask Yourself...
- Are you required to report the above scenario as potential child abuse?
- Why or why not?
- What about if this scenario had taken place at a playgroup meeting at the park and, instead of caring for this mother as a patient, she was a fellow parent who brought her child to play when you noticed the bruise and their poor relationship?
What to Expect When You Make a Report
For any mandated reporter who needs to call in suspected abuse, there is a specific hotline (1-800-635-1522) that may be called 24/7. There is also a hotline for non-mandated reporters (1-800-342-3720). You should call the line that best describes which capacity you are in when making the report (10). If you believe the child is in imminent danger, call 911.
All pertinent information should be gathered and readily available to make the call go as smoothly as possible. A written form (called LDSS-2221A) is available on the New York CPS website that can help gather all the necessary information. This paperwork must also be filled out and submitted within 48 hours of registering a verbal report (11).
Once connected with an agent, you will need to describe the child’s demographics, the scenario, and details that make you suspicious of abuse, the relationship of the person responsible for the suspected abuse, and where the child is now (11).
After information about the incident has been provided, the CPS agent will make one of three actions (11):
Report not registered
If the situation does not qualify for abuse, neglect, or maltreatment, a report may not be registered, and it may be recommended that the reporter connect the family with their local CPS department for services that may benefit them.
Law Enforcement referral
If the situation warrants immediate intervention by the police, such as if a crime is being committed or the child is in imminent danger, then the situation is reported to law enforcement. These situations are not registered as a report.
Report registered
If the situation meets the criteria for abuse, neglect, and maltreatment and does not require emergency action, it is registered as an official report and handed off to the appropriate local CPS agent for further investigation.
Once a report is registered, the local CPS agent will begin an investigation within 24 hours. During the investigation, the CPS agent will determine if the case is founded or unfounded (9).
- Unfounded reports are sealed and remain on record for ten years, after which they are expunged.
- Founded reports have 60 days for a plan of action to be created. CPS agents determine what sort of services, if any, a family should be connected with to improve the safety of the child or if removal from the home is warranted. Monitoring of these cases is ongoing.
Whenever a report is made, the caller is given a call ID number and can track the case’s progress at any time.
Self-Quiz
Ask Yourself...
- What sort of situation do you think would be considered imminent danger?
- Why do you think an imminent danger case gets referred to the police rather than registered as an official report?
- What sort of actions could be included in the plan for a founded report in order to improve the safety of a child’s home?
LDSS-2221A Form
The Report of Suspected Child Abuse or Maltreatment form known as LDSS-2221A, has several important elements that must be completed for the SCR to determine what actions need to be taken.
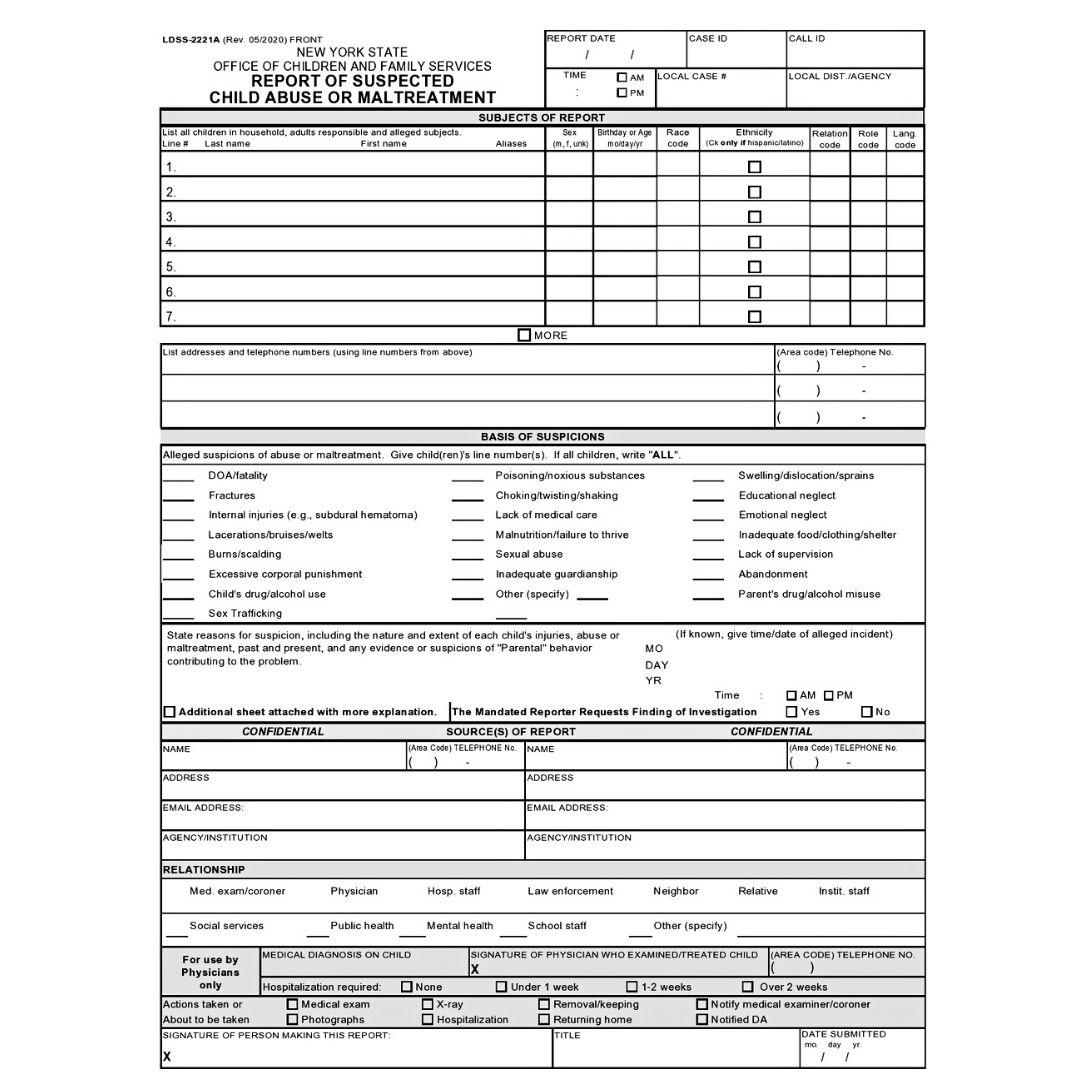
(12)
Section Breakdown
- List all children in the household, adults responsible, and alleged subjects.
- First and Last Name and known aliases.
- Sex
- Birthday or Age
- Race Code
- Ethnicity
- Relation Code
- Role Code
- Language Code
- List addresses and telephone numbers
- Basis of Suspicions
- The reporter will write the number of the child (from the list above) beside the following alleged suspicions, if all children, write all
- DOA/fatality
- Fractures
- Internal Injuries (e.g., subdural hematoma)
- Lacerations/bruises/welts
- Burns/scalding.
- Excessive corporal punishment
- Child’s drug/alcohol use
- Sex Trafficking
- Poisoning/noxious substances
- Choking/twisting/shaking
- Lack of medical care
- Malnutrition/failure to thrive.
- Sexual abuse
- Inadequate guardianship
- Swelling/dislocation/sprains
- Educational neglect
- Emotional neglect
- Inadequate food/clothing/shelter
- Lack of supervision
- Abandonment
- Parent’s drug/alcohol misuse
- Other (specify)
- State reasons for suspicion, including the nature and extent of each child’s injuries, abuse, or maltreatment, past and present, and any evidence or suspicions of “Parental” behavior contributing to the problem.
- Form provides space here for the reporter to explain, reporters can add an additional sheet with more information if there is not enough room.
- If the incident occurred on a specific date, provide the Month, Date, and Year
- Source(s) of Report
- The reporter will fill out their personal information in this section. Everything in this section will be strictly confidential but is necessary for CPS to obtain in case they need to contact the reporter for additional information regarding the case.
- Relationship
- This section refers to the reporter’s relationship with the child/children
- Medical examiner/coroner
- Physician
- Hospital staff
- Law enforcement
- Neighbor
- Relative
- Institutional staff
- Social services
- Public health
- Mental Health
- School Staff
- Other (specify)
- For use by Physicians only
- Medical diagnosis of child
- Signature of the physician who examined/treated the child.
- Telephone number
- The following are checkboxes:
- Hospitalization required.
- None
- Under 1 week
- 1-2 weeks
- Over 2 weeks
- Actions taken or about to be taken.
- Medical Exam
- Photographs
- X-ray
- Hospitalization
- Removal/keeping.
- Returning home
- Notify the medical examiner/coroner.
- Notified DA (12).
- Hospitalization required.
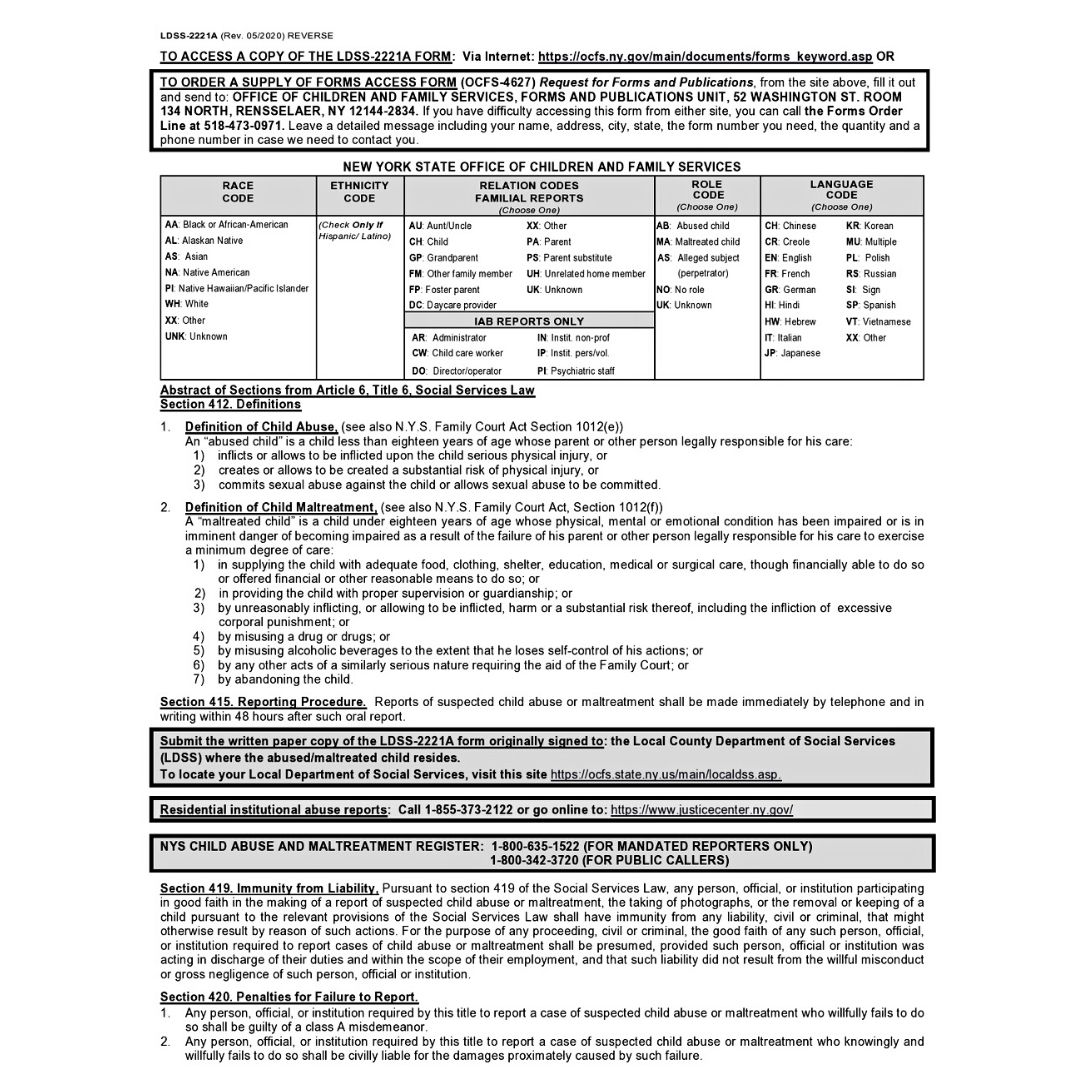
Page 2 (codes are explained in this section)
Page 3 provides additional space to write an explanation or provide pertinent information.
Legal Considerations
There are several legalities to consider regarding mandated reporters. The law is designed to protect those doing the reporting and encourage them to do so, even penalizing those who knowingly ignore abusive situations.
The main legal considerations for registering an abuse report include:
Immunity
One of the biggest concerns many mandated reporters have is what sort of liability or retaliation they might face after making a report. The law is very specific in that it protects anyone who makes a report in good faith, even if the investigation does not confirm abuse occurred.
In general, mandated reporters are immune from any legal action taken against them by a suspected abuser or employer who may be angered by the report. If an accused person believes a report was made in “bad faith” or as an attempt to knowingly falsify information that would incriminate them, they will have to prove this to be true in order for action to be taken against the mandated reporter.
Healthcare professionals reporting suspected abuse are not considered to be in violation of patient confidentiality laws either and may share patient information when it is done to protect the health and safety of a suspected victim of abuse. Employers may not keep employees from making reports or retaliate against them after a report has been made (9).
Confidentiality
The Office for Children and Family Services and Child Protective Services must keep the mandated reporter’s identity confidential and not release information about who or where a report came from whenever possible. This is intended to protect the mandated reporter from any negative attention, harassment, or social consequences of registering a report.
Mandated reporters are not required to inform parents when they are making a report, though they may choose to. Certain entities, such as police, attorneys, and other court officials, may request and be given information about who initiated a report in qualifying instances. For healthcare professionals who will need to testify in a court case, their identity cannot usually remain confidential (8).
Penalties
In addition to the protections offered to mandated reporters, there are also consequences for not reporting. Failing to report suspected abuse can be considered a Class A Misdemeanor and is punishable with up to 12 months in jail and/or a $1,000 fine. If serious injury or death befalls a child due to a lack of proper reporting, the mandated reporter can also be sued in civil court for damages or wrongful death.
It is important to remember that mandated reporters are only required to report suspected abuse that they encounter within their job duties and not outside of work or in their personal lives, though reporting even then is still encouraged (9).
Additional Information
Record requests may also be made of healthcare professionals who have made reports. Providing further information from a patient’s chart, including progress notes, records, diagnosis and treatment plans, or additional information about a patient is considered to be part of the SCR report and bypasses HIPAA laws. Providing this additional information is protected under the law as detailed above (9).
It is important to note that in order for the above protections to be upheld and to avoid penalties for not reporting, all reports must be made to the SCR and not to local law enforcement agencies or local social service departments. The SCR is used statewide and will contact local agencies, as necessary. Still, it is their responsibility, not the mandated reporters, to handle those resources once a report has been made (9).
Case Study
A 5-year-old patient is brought to the pediatric office with complaints of arm pain x 1 week. The mother states she was not with him but that he fell out of a swing in the backyard, and she assumed he was fine. When he continued to complain she decided to make an appointment a week later but thinks he is dramatic. She also later says he fell off a slide. An x-ray reveals a radial fracture, and the arm is in a cast.
You make a report to the SCR due to delay in seeking treatment, parental lack of concern, and inconsistent story. The investigation reveals no concern for abuse, and the case is closed. However, the mother is angry that a report was made and asked to speak to the supervisor of the department.
Self-Quiz
Ask Yourself...
- Are you liable for disciplinary action since no abuse was found?
- If the mother called CPS to ask who made the report, would they be required to tell her?
Adverse Childhood Experiences
Adverse Childhood Experiences or ACE is an umbrella term to describe events that had a potentially traumatic impact and that occurred before the individual turned 18 (3).
The CDC reports that approximately 64% of adults in the United States have experienced an ACE These experiences can have long-lasting effects on health, overall wellbeing, access to higher education, and job opportunities. The impact reaches far beyond just the individual, it can affect their family dynamics and can have societal implications. This is why preventing childhood abuse and promoting family stability needs to be a community effort and not just the responsibility of a select few (3).
Potential Impact of ACEs:
- Limited opportunities for higher education
- Limited financial resources
- Less access to job opportunities
- Unsafe sex practices – increased exposure to HIV and other STDs
- Substance and alcohol use
- Increased risk of cancer and diabetes
- Unintended pregnancy
- Mental health disorders such as depression, anxiety, PTSD, and suicidal ideation.
- Traumatic Brain Injury
- Fractures
- Burn injuries (3).
Community Strategies to Prevent ACE
- Increasing opportunities for families to have financial stability.
- Providing education on how to prevent violence and how to approach these situations as a person required to report or person encouraged to report.
- Community Youth Activities
- Early Intervention
- Affordable access to high-quality childcare (3).
Self-Quiz
Ask Yourself...
- What other negative impact can ACEs have on an individual?
- Thinking on community strategies, do you know of any opportunities or activities in your community that could help prevent ACE?
- Do you think that people who have experienced ACE are more likely to be perpetrators in the future? Why or why not?
Protective Factors to Prevent Child Abuse/Neglect
-
Nurturing and Attachment
Creating emotional bonds and attachments between parents and children in the early stages of development is very important. Research shows that this helps promote trust, feelings of love, acceptance, and protection. Children who experience consistent nurturing and attachment experiences tend to have more positive outcomes later in their adult lives (4).
-
Knowledge of parenting for child and youth development
Providing children with consistent, reasonable rules, expectations and opportunities leads to healthy child development that will allow them to succeed later in life. Positive parenting that demonstrates respect and love for children, rather than harsh punishments and unreasonable expectations, can be learned and there are many resources available for parents. (4).
-
Parental resilience
Dealing with the everyday stressors of life and being a parent can be very challenging at times. Learning healthy coping skills, developing resilience, strength and having flexibility when things don’t go quite as we expect them to can make a big difference in how we react towards children. Some people really struggle with this and lash out at their family and children, which is why this is included as a protective factor (4).
-
Social Connections
It really does take a village when it comes to raising children, parents can’t do it all alone. Having a strong support system of family, friends, and neighbors that you can turn to when you need advice or tangible help can really help reduce stress and anxiety. Parents with strong support systems are less likely to mistreat their children (4).
-
Concrete support for parents
This can include food assistance, help with childcare, job assistance programs, housing vouchers, and more. It’s important to connect parents who are in need with support networks and resources that will help them provide for their needs and for the needs of their children (4).
-
Social and emotional competence of children
Modeling how to communicate your emotions in a healthy, effective way, regulate your emotions, and nurture friendships and social connections will help develop social-emotional competence in the child (4).
Self-Quiz
Ask Yourself...
- What resources can you think of that can help parents with protective factor #2?
- What community and state-wide support programs can you think of? Do you think there is a need for more funding and support for these programs?
Special Populations
Limited English Proficiency (LEP)
LEP is defined as the limited ability to speak, read, or write English. It is essential to provide appropriate language assistance services to individuals with limited English proficiency. Healthcare institutions and other entities that receive any kind of federal funding are mandated by law to provide these services when indicated (11).
Indian Child Welfare Act
The purpose of this legislation is to support Native American, Indigenous, and First Nations children’s cultural identity when it comes to foster care placement, parental rights termination, emergency removals due to safety concerns, and adoption. CPS will work with the child’s tribe/nation regarding court proceedings and placements (11).
Immigrant Families
Investigations of suspected abuse or maltreatment will be conducted using the same standards as any other report. Not being a documented citizen is not grounds for the removal of the child or children in the household. CPS and mandated reporters should examine their own biases towards individuals who are not documented citizens and not be judgmental in these sensitive situations (11).
Self-Quiz
Ask Yourself...
- Is the use of qualified medical interpreters encouraged at your place of work? Do you know how to access these services to communicate with your patients?
- Immigrant families are treated with the same standards and guidelines as any other families, prior to reading this lesson, did you think otherwise? Why do you think you had that misconception?
Reducing Bias
Implicit bias is a subconscious attitude or opinion about a person or group of people that has the potential to influence the actions and decisions taken when providing care. Explicit bias is a conscious and controllable attitude (using racial slurs, making sexist comments, etc.) (8).
Before making a report, it is helpful to ask yourself these questions:
- Why am I suspecting abuse, neglect, or mistreatment?
- Is there objective evidence that supports my suspicion?
- Are the families’ values, race, cultural identity, or religion affecting how I perceive this situation? Would I feel the same if the family was more like mine? (13).
Research shows that implicit and explicit bias from healthcare providers exists, with Asian and Hispanic children’s cases of abuse being underreported, and cases of Black children being overrepresented in reports (13).
So how can we help mitigate bias in child abuse reporting? The number one thing we can do is to encourage ongoing and consistent evidence-based implicit bias education. Secondly, having standardized tools, protocols, and guidelines can help caseworkers and mandated reporters make sound decisions using critical thinking. Additionally, we must ensure we try to recognize how our own biases can have an impact on our decisions and work on increasing our knowledge (13).
We do not cover implicit bias at length in this course but do encourage you to seek out courses and training on this subject to increase your knowledge.
Self-Quiz
Ask Yourself...
- Does your workplace require implicit bias training?
- Think about the facility where you work and the different types of clients you encounter each day. Are there certain types of people you assume things about just based on the way they look, their gender, or their skin color?
- In what ways do you think these assumptions might affect the way you care for your patients, even if you keep these opinions internal?
- How do you think you could try and re-frame some of these assumptions?
Resources offered by the NY OFCS: excerpt from CPS Manual
OCFS H.E.A.R.S. – Help, Empower, Advocate, Reassure, and Support is a family line that assists families by providing resources and referrals to a variety of services. Families can call their helpline at 888-554-3277.
NY Project Hope provides emotional support for New York State residents.
Emotional Support Helpline (1-844-863-9314),
Online Wellness Groups, and a website filled with supportive resources (NYProjectHope.org).
The New York State Office for the Prevention of Domestic Violence
Prevent Child Abuse New York also has a prevention and parent helpline available for parents and caregivers. Families can call the helpline at 1-800-CHILDREN.
United Way – families can call 2-1-1, operated by the United Way, for health and human services information, referrals, assessments, and crisis support.
NYS Mandated Reporter site has additional resources
Conclusion
Though child abuse is an uncomfortable topic, most people who work in healthcare will encounter a situation sooner or later that raises concern and requires further action to promote young patients’ safety and well-being. With an improved understanding of who is at risk, key indicators to watch for, what sort of situations warrant reporting, and the reporting process itself, the hope is that abuse situations can be recognized and corrected early on, improving the health and safety of New York’s children as much as possible.
References + Disclaimer
- American Society for the Positive Care of Children. (2020). Child abuse statistics in the U.S. Retrieved from: https://americanspcc.org/child-abuse-statistics/
- American Society for the Positive Care of Children. (2020). Indicators of child abuse. Retrieved from: https://americanspcc.org/indicators-child-abuse/
- Centers for Disease Control and Prevention (2023). Fast Facts: Preventing Adverse Childhood Experiences. Retrieved on July 27th, 2023, from https://www.cdc.gov/violenceprevention/aces/fastfact.html
- Child Welfare Information Gateway (2020). Protective Factors Approaches in Child Welfare. Retrieved on September 7th, 2023, from https://www.childwelfare.gov/topics/preventing/promoting/protectfactors/
- Child Welfare League of America. (2017). New York’s children at a glance. Retrieved from: https://www.cwla.org/wp-content/uploads/2017/04/NEW-YORK-.pdf
- Family Court Act. (n. d.) Article 10: child protective proceedings. Retrieved from: https://www.nysenate.gov/legislation/laws/FCT/A10
- FitzGerald, C., and Hurst, S. (2017). Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics, 18, 19. https://doi.org/10.1186/s12910-017-0179-8
- National Children’s Alliance. (2020). National child abuse statistics. Retrieved from https://www.nationalchildrensalliance.org/media-room/national-statistics-on-child-abuse/
- New York Consolidated Law- Social Services. (2019). SOS 411-428 Child protective services. Retrieved from: https://law.justia.com/codes/new-york/2012/sos/article-6/title-6/415/
- New York Kid’s Well-being Indicators Clearinghouse. (2020). Child abuse and maltreatment. Retrieved from: https://www.nyskwic.org/get_data/indicator_profile.cfm?subIndicatorID=107
- New York State Office of Children and Family Services. (n.d.). Child protective services. Retrieved from: https://ocfs.ny.gov/programs/cps/#:~:text=The%20purpose%20of%20the%20Child,each%20county%20in%20New%20York.
- NY Office of Children and Family Services (2022). New York State Child Protective Services Manual. Retrieved on September 6th, 2023, from https://ocfs.ny.gov/programs/cps/manual/
- Palusci, V., Botash, A. (2021). Race and Bias in Child Maltreatment Diagnosis and Reporting. Pediatrics July 2021; 148 (1): e2020049625. 10.1542/peds.2020-049625 Retrieved from https://publications.aap.org/pediatrics/article/148/1/e2020049625/179923/Race-and-Bias-in-Child-Maltreatment-Diagnosis-and?autologincheck=redirected
- University of South Carolina (2020). Virtual Settings: Recognizing and Reporting Child Abuse & Neglect. Retrieved on September 7th 2023 from https://dc.statelibrary.sc.gov/bitstream/handle/10827/35104/CLC_Virtual_Settings_Recognizing_And_Reporting_Child_Abuse_2020-07.pdf?sequence=1&isAllowed=y
Disclaimer:
Use of Course Content. The courses provided by NCC are based on industry knowledge and input from professional nurses, experts, practitioners, and other individuals and institutions. The information presented in this course is intended solely for the use of healthcare professionals taking this course, for credit, from NCC. The information is designed to assist healthcare professionals, including nurses, in addressing issues associated with healthcare. The information provided in this course is general in nature and is not designed to address any specific situation. This publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals. Hospitals or other organizations using this publication as a part of their own orientation processes should review the contents of this publication to ensure accuracy and compliance before using this publication. Knowledge, procedures or insight gained from the Student in the course of taking classes provided by NCC may be used at the Student’s discretion during their course of work or otherwise in a professional capacity. The Student understands and agrees that NCC shall not be held liable for any acts, errors, advice or omissions provided by the Student based on knowledge or advice acquired by NCC. The Student is solely responsible for his/her own actions, even if information and/or education was acquired from a NCC course pertaining to that action or actions. By clicking “complete” you are agreeing to these terms of use.
➁ Complete Survey
Give us your thoughts and feedback
➂ Click Complete
To receive your certificate